
Gene for Calcium Channel Linked to Bipolar Disorder in Several Ways

No one gene explains the risk of developing bipolar disorder. Many genes are involved, each with a small effect. However, the effects of one particular gene have been validated in multiple different ways. The gene is called CACNA1C, and it codes for one subunit of the dihydropyridine L-type calcium channel. Calcium channels are structures on the membranes of neurons that allow calcium to enter cells and alter their excitability.
Different people can have different variants of the CACNA1C gene, depending on which nucleotides appear there: valine (Val) or methionine (Met). One particular variant (known as the Met/Met single nucleotide polymorphism, rs1006737) has been associated with executive function deficits compared to the Val/Val variant in multiple tests in patients with bipolar disorder. Executive function refers to abilities like planning, organizing, and retaining information. This was reported by Soeiro-de-Souza et al. in the journal Acta Psychiatrica Scandinavica in 2013.
Importantly, CACNA1C has also been linked to risk of bipolar disorder, a finding that was replicated in several large genome-wide association studies (GWAS). Autopsy studies of people who had been diagnosed with bipolar disorder show more calcium channels in their brains. The Met/Met variant of the CACNA1C gene also lets more calcium ions into cells. Those who have the gene variant also show differences in some brain structures known to be involved in the modulation of emotions compared to those without the variant.
In addition to these findings, more than a dozen studies report increased intracellular calcium in the white blood cells of people with bipolar disorder compared to controls. To the extent that these increases in intracellular calcium reflect changes in neurons, this would be consistent with the findings about CACNA1C. High levels of calcium influx and the associated intracellular calcium may increase cellular excitability and potentially dysregulate normal neuronal functioning.
The final piece of evidence linking altered calcium channel regulation to bipolar disorder is a direct therapeutic test of a drug that blocks calcium influx through the dihydropyridine L-type calcium channel. There is evidence that nimodipine, which selectively blocks dihydropyridine L-type calcium channels, has therapeutic effects in bipolar disorder.
Fear Memories Can Be Erased or Provoked in Animals

Researchers have identified neurons responsible for remembering conditioned fear in the amygdala of rodents, and can turn them on and off. At the 2013 meeting of the Society of Biological Psychiatry, Sheena A. Josselyn gave a breath-taking presentation on this process.
When animals hear a tone they have learned to associate with the imminent delivery of a shock in a given environment, they learn to avoid that environment, and they reveal their learning of the tone-shock association by freezing in place. Josselyn was able to observe that 20% of the neurons in the lateral nucleus of the amygdala were involved in this memory trace. They were revealed by their ability to increase the transcription factor CREB, which is a marker of cell activation. Using cutting-edge molecular genetic techniques, the researchers could selectively eliminate only these CREB-expressing neurons (using a new technology in which a diphtheria toxin is attached to designer receptors exclusively activated by designer drugs, or DREADDs) and consequently erase the fear memory.
The researchers could also temporarily inhibit the memory, by de-activating the memory trace cells, or induce the memory, so that the animal would freeze in a new context. Josselyn and colleagues were able to identify the memory trace for two different tones in two different populations of amygdala neurons.
The same molecular tricks with memory also worked with cocaine cues, using what is known as a conditioned place preference test. A rodent will show a preference for an environment where it received cocaine. Knocking out the selected neurons would remove the memory of the cocaine experience, erasing the place preference.
The memory for cocaine involved a subset of amygdala neurons that were also involved in the conditioned fear memory trace. Incidentally, Josselyn and her group were eventually able to show that amygdala neurons were in competition with each other as to whether they would be involved in the memory trace for conditioned fear or for the conditioned cocaine place preference.
Treating Substance Abuse: A Step Forward
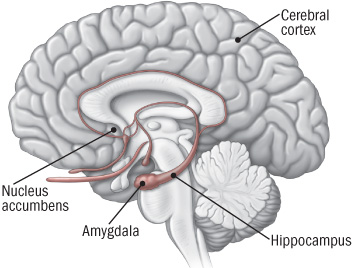 New discoveries in neuroanatomy are helping clarify what addiction looks like in the brain. Peter Kalivas of the Medical University of South Carolina reported at the 2013 meeting of the Society of Biological Psychiatry that most drugs of abuse alter glutamate levels and the plasticity of synapses in the nucleus accumbens, the reward area of the brain. Glutamate is the main excitatory neurotransmitter in the brain, and compulsive habits may be associated with increased release of glutamate in this brain area.
New discoveries in neuroanatomy are helping clarify what addiction looks like in the brain. Peter Kalivas of the Medical University of South Carolina reported at the 2013 meeting of the Society of Biological Psychiatry that most drugs of abuse alter glutamate levels and the plasticity of synapses in the nucleus accumbens, the reward area of the brain. Glutamate is the main excitatory neurotransmitter in the brain, and compulsive habits may be associated with increased release of glutamate in this brain area.
During chronic cocaine administration, for example, the neurons in the nucleus accumbens lose their adaptive flexibility and their ability to respond to signals from the prefrontal cortex. Normally, low levels of stimulation would induce long-term depression (LTD) while high levels of stimulation would induce long-term potentiation (LTP). These are long-term changes in the strength of a synapse, which allow the brain to change with learning and memory. When long-term potentiation and long-term depression are no longer possible, memory and new learning in response to messages from the prefrontal cortex are diminished.
Given this absence of flexible responding, animals extinguished from cocaine self-administration (when a lever they had pressed to receive cocaine ceases to provide cocaine) are highly susceptible to cocaine reinstatement if a stressor is presented or if a signal appears that suggests the availability of cocaine. This cocaine reinstatement is associated with high levels of glutamate in the nucleus accumbens, so Kalivas reasoned accurately that lowering these levels would be associated with a lesser likelihood of cocaine reinstatement.
The drug N-acetylcysteine (NAC), which is available from health food stores, decreases the amount of glutamate in the nucleus accumbens by inducing a glutamate transporter in glial cells that helps clear excess synaptic glutamate. In Kalivas’ research, NAC prevented cocaine reinstatement, cocaine-induced anatomical changes in spine shape (bigger, stubby spines), and the loss of long-term potentiation and long-term depression in the nucleus accumbens.
The findings on NAC in animal studies led to a series of important small placebo-controlled clinical trials in people with a variety of addictions, and positive results have been found using NAC in people addicted to opiates, cocaine, alcohol, marijuana, and gambling. It also decreases hair-pulling in trichotillomania and reduces stereotypy and irritability in children with autism.
NAC also appears to be effective in the treatment of unipolar and bipolar depressed patients in placebo-controlled trials by Australian researcher Michael Berk. Thus, NAC could be useful for patients with affective disorders who are also having difficulties with comorbid substance use.
Some antibiotics (that are not commonly available) also induce the glutamate transporter and glial cells of the nucleus accumbens, offering a potential new approach to treating some addictions.
Treatment Research Needs More Advocacy

Among the hundreds of posters, workshops, clinical perspectives, and symposia presented over five days at the 2013 meeting of the American Academy of Child and Adolescent Psychiatry (AACAP), there were almost no posters or presentations on new approaches to treatment (either with drugs or therapy) for children with bipolar disorder.
As we have repeatedly emphasized in the BNN and in research publications, this deficiency has adverse consequences for the many hundreds of thousands of children and adolescents in the US with unequivocal diagnoses of bipolar disorder. Suicide is now the second leading cause of death in adolescents 13 to 17 years of age in the US. Most of these young people have a mood disorder. Bipolar disorder carries with it not only a substantial risk of suicide, but also the potential for a lifetime of dysfunction, disability, and medical comorbidity if it is inadequately treated.
Please advocate for more treatment research for childhood onset bipolar disorder. A whole generation of children, their parents, and their physicians desperately need more treatment information.
Gene Mutation Induces Bipolar-Like Symptoms
A mutation in a gene related to circadian rhythms may help explain bipolar disorder. Animals with a mutation in the gene, known as CLOCK, typically exhibit behaviors that mimic human mania, such as increased locomotor activity and decreased anxiety.
Stress can lead to depression in bipolar patients, so researcher Nicole Edgar et al. exposed animals with the mutated “manic” version of the CLOCK gene to unpredictable chronic mild stress. The stress brought about decreased locomotor activity and increased anxiety, mimicking a switch into depression. These data suggest that alterations in CLOCK genes may provide a useful model for both mania and depression.
The research was presented at the 2013 meeting of the Society of Biological Psychiatry, and the abstract (#471) can be found in the meeting supplement, Volume 73, Number 9S of the journal Biological Psychiatry.
In another abstract (#472) at the same meeting, researcher Wilbur Williams et al. reported that alterations in related clock genes (that result in decreases in the proteins CRY-1 and SIRT1) are associated with manic-like behavior that could be reversed using lithium. These data further suggest that clock genes may provide a useful model for bipolar disorder.
High CRP Predicts Early Onset Of A Mood Episode
C-reactive protein
Barbara Gracious of Ohio State University became interested in the inflammatory marker CRP through studying vitamin D3 deficiency. Vitamin D is a neurosteroid, and low levels of it have been associated with risk of schizophrenia, cardiovascular disease (heart attack), diabetes, mood disorders, cognitive deficits, autoimmune disease, and obesity. High CRP levels are related to low vitamin D, to obesity, and to other inflammatory markers such as IL-6 and TNF alpha.
Gracious measured these levels of CRP in 621 children participating in the Longitudinal Study of Manic Symptoms (LAMS), who were followed up for many years. She found that those with higher levels of CRP developed a mood episode approximately two years earlier than those with normal levels. CRP binds phosphocholine, which activates complement, a kind of protein that induces inflammation. CRP is elevated in 14% to 53% of patients with depression and anxiety.
Copeland et al. reported in the American Journal of Psychiatry in 2012 that after a first depression, high CRP was associated with relapse. CRP also increases in adolescent females (who are at increased risk for depression).
Editor’s Note: These findings suggest the potential importance not only of using CRP as an indicator of depression risk, but also of targeting CRP levels in the hopes of reducing risk of a mood episode in children with elevated inflammatory markers. Supplementing vitamin D3 in those with low levels would be a good place to start, as would preventing or treating obesity and promoting good sleep hygiene and exercise. The potential role of medications with direct anti-inflammatory effects such as aspirin (acetylsalicylic acid) or minocycline deserves further study.
Balanced diet, exercise, and good sleep habits may be easier said (or recommended) than done. Such lifestyle advice must be delivered with motivational interviewing, and instilled through practice, positive feedback, encouragement, and more practice. In children in general, and especially in those at high risk for a mood episode due to a family history of a unipolar or bipolar mood disorder, starting things off right from the outset with good diet, exercise, and sleep routines would be highly recommended. The benefits for long-term health and wellbeing could be enormous.
The results of good health behaviors may be mediated through several pathways. They could lessen inflammation and obesity, increase brain-derived neurotrophic factor (BDNF, which is important for new synapses and long-term memory) and neurogenesis (both of which are increased by exercise), and even lengthen the telomeres that cap the ends of each strand of DNA (short ones are associated with a variety of medical and psychiatric illnesses).
Cognitive Behavioral Therapy Helps Depression And Inflammation In Inflammatory Bowel Disease
 Cognitive behavioral therapy may improve both depression symptoms and inflammatory bowel disease. At a symposium on early-onset depression at the 2013 meeting of the American Academy of Child and Adolescent Psychiatry, Eva Szigethy of the University of Pittsburg discussed depression in inflammatory bowel disease (IBD), i.e. Crohn’s disease or ulcerative colitis. Depression and bipolar disorder are often associated with elevated inflammatory markers, such as IL-1b, IL-2, IL-6, INF gamma, TNF alpha, and CRP (C-reactive protein). This kind of inflammation can cause symptoms like decreased appetite, fatigue, anhedonia (loss of pleasure in activities one once enjoyed), and motor slowing.
Cognitive behavioral therapy may improve both depression symptoms and inflammatory bowel disease. At a symposium on early-onset depression at the 2013 meeting of the American Academy of Child and Adolescent Psychiatry, Eva Szigethy of the University of Pittsburg discussed depression in inflammatory bowel disease (IBD), i.e. Crohn’s disease or ulcerative colitis. Depression and bipolar disorder are often associated with elevated inflammatory markers, such as IL-1b, IL-2, IL-6, INF gamma, TNF alpha, and CRP (C-reactive protein). This kind of inflammation can cause symptoms like decreased appetite, fatigue, anhedonia (loss of pleasure in activities one once enjoyed), and motor slowing.
In children with IBD randomized to cognitive behavioral therapy or just routine supportive care, the somatic symptoms of those receiving cognitive behavioral therapy improved, as did their IBD.
Other treatments may also target both depression and inflammation. Szigethy noted that there is some evidence that the TNF alpha–inhibiting anti-inflammatory drug infliximab has some antidepressant effects in those with high CRP and in patients with the autoimmune condition psoriasis. She indicated that the antidepressant bupropion decreases depression and inflammation in IBD and that bupropion has anti–TNF alpha effects (at least in animals).
Currently levels of inflammation are measured with blood drawn from a vein, but new techniques may be more child-friendly. These include measuring inflammatory markers in hair (which reflects levels over the previous two weeks), saliva, or with a drop of blood from a pinprick (as used by researcher Ben Goldstein).
Cognitive Behavioral Therapy Tailored For Children and Adolescents

At a symposium on early-onset depression at the 2013 meeting of the American Academy of Child and Adolescent Psychiatry, Betsy Kennard described a course of cognitive behavioral therapy tailored to eliminating residual symptoms in children with unipolar depression who had no family history of a parent with bipolar disorder. In the same study Graham Emslie discussed, the investigators considered cognitive behavioral therapy for the treatment of childhood- and adolescent-onset depression.
The therapy was aimed at achieving health and wellbeing and focusing on positive attributes and strengths in the child, and it was designed to be a shorter than usual course (i.e. four weekly sessions, then four every other week, and one at three months). This regimen typically also included three to five family sessions. Other key components of the therapy included anticipating and dealing with stressors, setting goals, and practicing all the skills learned.
On a visual timeline, children identified and wrote down past stressors, how they felt when depressed, their automatic cognitions, ways they would know when they were feeling down again (i.e. feeling isolated, angry at parents, etc.), their strengths and skills, what obstacles to feeling better existed and how to circumvent them, and their long-term goals.
The therapy was based on the research of Martin Seligman and Giovanni A. Fava, plus Rye’s Six S’s (soothing, self-healing, social, success, spiritual, and self-acceptance). The children participated in practice and skill-building in each domain. Sleep hygiene and exercise were emphasized. The idea of “making it stick” was made concrete with phrases on sticky notes taken home and put up on a mirror. Postcards were even sent between sessions as reminders and for encouragement.
Editor’s Note: Most depressed kids don’t get completely well (only about 20% after an acute course of medication). Something must be added. This kind of specialized cognitive behavior therapy works and keeps patients from relapsing. This study included only those children with unipolar depression whose parents did not have bipolar disorder. However, Emslie noted that depressed children of a bipolar parent also had an exceedingly low rate of switching into mania (2 to 4%) in his experience, so fluoxetine followed by cognitive behavioral therapy might be considered for treating unipolar depressed children of a bipolar parent.
Once children have developed bipolar disorder, evidenced by hypomania or mania followed by depression, antidepressants are to be avoided in favor of mood stabilizers and atypical antipsychotics, since there is a higher switch rate in these youth when they are prescribed antidepressant monotherapy.
Since children with bipolar disorder are at such high risk for continued symptoms and relapses, the strategy of adding cognitive behavioral therapy to their successful drug treatment would appear appropriate for them as well as those with unipolar depression, especially since there is a large positive literature on the efficacy of cognitive behavioral therapy, psychoeducation, and Family Focused Therapy (FFT) in children and adults with bipolar depression. As noted previously, FFT is very effective for children at high risk because of a parent with bipolar disorder and who are already symptomatic with anxiety, depression or BP-NOS.
Moral of the story: getting kids with unipolar or bipolar depression well and keeping them well is a difficult endeavor that requires specialized, combined medication and therapy approaches and follow-up education and therapy. This is for sure. The hope would also be that good early and long-term intervention would yield a more benign course of recurrent unipolar or bipolar disorder than would treatment as usual (which all too often consists of medication only).
Continuation Cognitive Behavioral Therapy Prevents Relapse in Kids

At a symposium on early-onset depression at the 2013 meeting of the American Academy of Child and Adolescent Psychiatry, Graham Emslie of the University of Texas Southwestern Medical Center discussed the role of cognitive behavioral therapy in the long-term treatment of child-and adolescent-onset unipolar depression.
In Emslie’s research, the combination of the antidepressant fluoxetine and cognitive behavioral therapy reduced depressive relapses in children. Using the two treatments together did not speed onset of antidepressant response compared to fluoxetine alone, but once children responded to the medication, the addition of cognitive behavioral therapy reduced relapses over the next year compared to fluoxetine alone (even though the cognitive behavioral therapy ended after the first six months).
Emslie likened the use of cognitive behavioral therapy to the course of rehabilitation that often follows a major surgery and is meant to sustain or enhance the good effects of surgery. Getting patients to full remission (well and with no residual symptoms) was the key to staying well.
Rationale for Using Ketamine in Youth with Treatment-Resistant Depression

At the 2013 meeting of the American Academy of Child and Adolescent Psychiatry, Vilma Gabbay of the Mount Sinai School of Medicine reiterated the findings from the TORDIA (Treatment of SSRI-Resistant Depression in Adolescents) study that 20% of young people with depression remained resistant to treatment, childhood-onset depression was more likely to be recurrent and more difficult than adult-onset depression in the long run, and suicide was the second leading cause of death in 12- to 17-year-olds in 2010 according to a Centers for Disease Control report in May 2013. Anhedonia (a loss of pleasure in activities once enjoyed) was the most difficult symptom to treat in adolescents.
Gabbay carefully explained some of the rationales for using ketamine in young people with depression. The presence of inflammation is a poor prognosis factor, and ketamine has anti-inflammatory effects, decreasing levels of inflammatory markers CRP, TNF-alpha, and Il-6.Given that ketamine has been widely used as an anesthetic for surgical procedures, its safety in children has already been demonstrated. Ketamine did not appear to cause behavioral sensitization (that is, increased effect upon repetition) in a report by Cho et al. in 2005 that included 295 patients.
As noted previously, Papolos et al. reported in a 2012 article in the Journal of Affective Disorders that intranasal ketamine at doses of 50 to 120 mg was well-tolerated and had positive clinical effects in 6- to 19-year-olds with the fear of harm subtype of bipolar disorder that had been highly resistant to treatment with more conventional drugs.
Gabbay reluctantly endorsed further cautious controlled trials in children and adolescents, in light of ketamine’s suggested efficacy and good safety profile, which stands in contrast to its popular reputation as a party drug or “Special K.”
Editor’s Note: The discussant of the symposium, Neal Ryan of Western Psychiatric Institute and Clinic, added an exquisitely brief discussion suggesting that ketamine should ultimately be studied in combination with behavioral and psychotherapeutic procedures to see if its therapeutic effects could be enhanced. He made this suggestion based on the data that ketamine has important synaptic effects, increasing brain-derived neurotrophic factor (BDNF), which is important for healthy cells and long-term memory, and reverting thin dendritic spines caused by stress back to their normal mushroom shape. This editor (Robert Post) could not be more in agreement.
