
Accelerated Intermittent Theta-Burst Stimulation (aiTBS) Quickly Improved Treatment-Resistant Depression

At the 2021 meeting of the Society of Biological Psychiatry (SOBP), researcher Nolan Williams and colleagues described a sham-controlled trial of accelerated intermittent theta-burst stimulation (aiTBS) in patients with treatment-resistant depression. Theta burst stimulation is a specific protocol for rTMS, or repeated transcranial magnetic stimulation, a non-invasive form of brain stimulation. Magnets placed on a patient’s head provide bursts of high-frequency stimulation to the brain.
Participants in the study received 50 sessions over 5 days of either aiTBS or a sham procedure. Among those who received the real aiTBS treatment, 85.7% saw an improvement in their treatment-resistant depression, compared to only 26.7% of those in the sham group. AiTBS produced a rapid antidepressant response, which Williams and colleagues suggest could be useful for the treatment of patients in emergency rooms or inpatient settings.
Transcranial Near-Infrared Light May Treat Brain Injury and Neurodegeneration
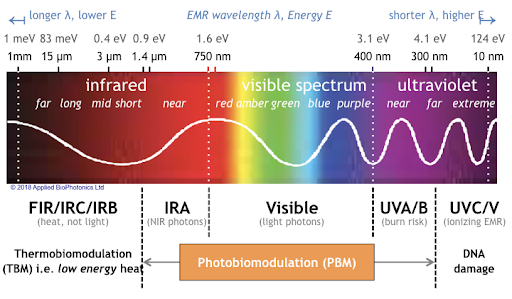
At the 2021 meeting of the Society of Biological Psychiatry, there was a symposium on treatment with near-infrared light chaired by researchers Paolo Cassano and Dan Iosifescu. The treatment is known as transcranial photobiomodulation (PBM) with near-infrared light. A device worn on the head delivers infrared light that penetrates the cerebral cortex and can modulate cortical excitability. It has a variety of effects including promoting neuroplasticity, improving oxygenation, and decreasing inflammation and oxidative stress.
A number of studies exploring the possibility that PBM could be used as a clinical treatment for conditions such as depression, brain injury, or dementia were presented at the symposium.
Researcher Lorelei Tucker discussed promising findings from an animal model in which rats with stroke or brain injuries showed improvement after being treated with PBM.
Cassano discussed studies aimed at refining which brain areas should be targeted with PBM and how much light should be delivered in order to improve depression. In double-blind, sham-controlled studies in people with major depression, targeting the dorsolateral prefrontal cortex with PBM improved their symptoms.
Researcher Benjamin Vakoc discussed a study of low-level light therapy (LLLT) using near-infrared light compared to a sham procedure in 68 people with moderate traumatic brain injury. The researchers used magnetic resonance imaging (MRI) to assess changes in white matter in the brain over time in people recovering from an acute brain injury. Patterns of changes in white matter were different for those who received LLLT compared to those who received the sham procedure.
Researcher Linda Chao described a very small study to determine whether PBM could improve symptoms of dementia. Four patients received typical dementia care while four others underwent home treatments with the commercially available Vielight Neuro Gamma device, which delivers PBM via both the scalp and an insert in the nose. After 12 weeks, the PBM group showed improvements in cognition and brain connectivity.

Editor’s Note: We will be watching the literature to follow advances in this promising novel method of neuromodulation.
Participation in Sports May Mitigate Genetic Risk for ADHD in School-Aged Children

At the 2021 meeting of the Society of Biological Psychiatry, researcher Keiko Kunitoki and colleagues reported that participation in sports decreased behavior abnormalities in 9- and 10-year-old children at genetic risk for attention deficit hyperactivity disorder (ADHD). Sports were associated with greater hippocampal volume, which was associated with fewer behavioral abnormalities. Kunitoki and colleagues concluded that “participation in team sports mitigated genomic risk for psychopathology at age 9–10 in part through increased hippocampal volume.”
Editor’s Note: These data are consistent with a program called the Vermont Family-Based Approach developed by researcher James Hudziak, who heads the Vermont Center for Children, Youth and Families at the University of Vermont. The program encourages families to practice different domains of wellness, such as music, mindfulness, exercise, and nutrition, among others. The idea is to support emotional and behavioral health, and to do so intensively in families where children show signs of mood and behavioral difficulties or are at risk for these difficulties.
Hudziak analyzed brain scans of 232 children aged 6 to 18 and reported that “practicing an instrument such as the piano or violin increased working memory, gray matter volume in the brain, and the ability to screen out irrelevant noise. Practicing mindfulness increased white matter volume and reduced anxiety and depression. Exercise also increased brain volume and neuropsychological abilities.”
In 2015, researcher Benjamin I. Goldstein reported that 20 minutes of vigorous exercise on a bike improved cognition and decreased hyperactivity in the medial prefrontal cortex in adolescents with and without bipolar disorder, and researcher Danella M. Hafeman reported that offspring of parents with bipolar disorder who exercised more had lower levels of anxiety.
To summarize, engaging in exercise, team sports, music, and meditation/mindfulness are beneficial for all children, and can be especially helpful for those at risk for depression or bipolar disorder. Children who are already symptomatic should additionally be offered something like family focused therapy (FFT), a multi-faceted approach developed by researcher David Miklowitz, in which families of young people at risk for bipolar disorder take part in therapy, learning together about the illness and practicing strategies for communication and coping.
Surface Area of Cortex Is Reduced After Multiple Manic Episodes
In a 2020 article in the journal Psychiatric Research: Neuroimaging, researcher Rashmin Achalia and colleagues described a study of structural magnetic resonance imaging (MRI) that compared 30 people with bipolar I disorder who had had one or several episodes of mania to healthy volunteers. Compared to the healthy volunteers, people with bipolar disorder had “significantly lower surface area in bilateral cuneus, right postcentral gyrus, and rostral middle frontal gyri; and lower cortical volume in the left middle temporal gyrus, right postcentral gyrus, and right cuneus.”
The surface area of the cortex in patients with bipolar I disorder who had had a single episode of mania resembled that of the healthy volunteers, while those who had had multiple manic episodes had less cortical surface area.
The data suggest that compared to healthy volunteers, people with bipolar disorder have major losses in brain surface area after multiple episodes that are not seen in first episode patients. In addition, the researchers found that both the number of episodes and the duration of illness was correlated with the degree of deficit in the thickness in the left superior frontal gyrus. These decreases in brain measures occurred after an average of only 5.6 years of illness.
Editor’s Note: These data once again emphasize the importance of preventing illness recurrence from the outset, meaning after the first episode. Preventing episodes may prevent the loss of brain surface and thickness.
Clinical data has also shown that multiple episodes are associated with personal pain and distress, dysfunction, social and economic losses, cognitive deficits, treatment resistance, and multiple medical and psychiatric comorbidities. These and other data indicate that treatment after a first episode must be more intensive, multimodal, and continuous and include expert psychopharmacological and psychosocial support, as well as family education and support. Intensive treatment like this can be life-saving. The current study also supports the mantra we have espoused: prevent episodes, protect the brain and the person.
Left Prefrontal Strokes Linked to Depression

In a 2021 article in the journal Stroke, researcher Julian Klingbeil and colleagues reported that left, but not right, ventrolateral prefrontal stroke lesions were associated with increased risk of depression at six months post-stroke.
The study included 270 participants who had their first-ever stroke. Six months following their strokes, 19.6% of the participants had depression. Those who scored higher on a scale of depression and anxiety symptoms in the first month after their stroke were more likely to have depression six months after the stroke.
The researchers identified a cluster of locations for stroke lesions, mostly within the left ventrolateral prefrontal cortex, that they linked to depression symptoms six months post-stroke. Klingbeil and colleagues hope that recognizing lesions in this region as risk factors for depression will help with early diagnosis of depression among people who recently had a stroke.
Editor’s Note: Antidepressants have been shown to improve post-stroke recovery of neurological functional (and depression) that is caused by the cutoff of blood supply during a stroke (ischemia). Patients and their family members should talk with their neurologist about treatment of ischemic strokes with antidepressants, especially when the lesions occur on the left side of the brain.
Psychiatric Disorders Linked to More Physical Disease

In an article in the journal JAMA Network Open, Leah S. Richmond-Rakerd and colleagues found that people with mental disorders had more physical disease at younger ages, they had more and longer hospitalizations and associated health care costs, and they were more likely to die at younger ages than people without mental disorders.
The research came from a population-based cohort study of more than 2.3 million citizens of New Zealand over three decades. The authors concluded, “These findings suggest that ameliorating mental disorders may have implications for improving the length and quality of life and for reducing the health care costs associated with physical diseases.”
Editor’s Note: This editor would suggest the importance of also doing the opposite, that is, looking out for and treating and preventing the physical illnesses to which psychiatric patients are more vulnerable in order to improve the length and quality of life.
Either way, medical illnesses, both physical and psychiatric, are intimately intertwined, and both deserve careful and early intervention. Psychiatric and physical illnesses cause suffering, disability, and early demise. Major psychiatric illnesses need to be seen as potentially lethal medical illnesses, a fact that few people realize. Conversely, physical illnesses are often not treated as aggressively or intensively in psychiatric patients as in the general population. For example, patients with bipolar disorder get fewer interventions with stents and bypasses for the same heart problems as others. Special attention needs to be given to better encourage and support the medical health of psychiatric patients.
ADHD Common in People with Mood Disorders

In a meta-analysis published in the journal Acta Psychiatrica Scandinavica in 2021, researcher Andrea Sandstrom and colleagues reported that people with mood disorders had a three times higher incidence of attention-deficit hyperactivity disorder (ADHD) than people without mood disorders. ADHD was also more likely to occur in people with bipolar disorder than in people with major depression. The comorbidity is most common in childhood, less so in adolescence, and lowest in adulthood.
Based on 92 studies including a total of 17,089 individuals, the prevalence of ADHD in people with bipolar disorder is 73% in childhood, 43% in adolescence, and 17% in adulthood. Data from 52 studies with 16,897 individuals indicated that prevalence of ADHD in major depressive disorder is 28% in childhood, 17% in adolescence, and 7% in adulthood.
Editor’s Note: A key implication of this research is that there is a huge overlap of bipolar disorder and ADHD in childhood, and that physicians need to specifically look for bipolar symptoms that are not common in ADHD to make a correct diagnosis. These include: brief or extended periods of mood elevation and decreased need for sleep in the youngest children; suicidal or homicidal thoughts and threats in slightly older children; hyper-sexual interests and actions; and hallucinations and delusions. When these are present, even when there are also clear-cut ADHD symptoms, a clinician must consider a diagnosis of bipolar disorder and treat the child with mood stabilizers prior to using stimulants or other traditional ADHD medications.
Conversely, physicians should be aware of the much lower incidence of ADHD in adolescents and adults with bipolar disorder. Here one should first make sure that the apparent ADHD symptoms of hyperactivity, inattention, poor concentration, etc. do not result from inadequately treated mania and depression, and if they do, treat these symptoms to remission prior to using traditional ADHD medications.
Study Examines Comorbidity of ADHD and Bipolar Disorder

In a 2021 review and meta-analysis in the journal Neuroscience and Biobehavioral Reviews, researcher Carmen Schiweck and colleagues described the comorbidity of attention-deficit hyperactivity disorder (ADHD) and bipolar disorder in adults. This was the first review and meta-analysis to quantify the comorbidity of the two fairly prevalent disorders. The meta-analysis included 71 studies with a combined total of 646,766 participants from 18 countries.
The review found that among people with ADHD, about 1 in 13 also have bipolar disorder, while among people with bipolar disorder, 1 in 6 have comorbid ADHD. The prevalence differed depending on the continent where patients lived and the diagnostic systems used there, with greater prevalence of both disorders in the US, where the Diagnostic and Statistical Manual of Mental Disorders is used, than in Europe, where the International Classification of Diseases is typically used. (Other parts of the world were less represented in the meta-analysis.) Schiweck and colleagues found that bipolar disorder had an onset about 4 years earlier in patients who had comorbid ADHD.
Insomnia Plays Critical Role in Bipolar Disorder

In a 2021 article in the Journal of Psychiatric Research, researcher Laura Palagini and colleagues reported that insomnia symptoms can affect the course of bipolar illness. In a helpful summary and interview in the Psychiatry & Behavioral Health Learning Network’s Psych Focus, she stated that:
“1) BD patients in a depressive phase with clinically significant insomnia met a greater severity not only of depressive symptoms and suicidal risk, but also of early life stressors and the cognitive part of hopelessness, compared with patients without insomnia
“2) insomnia symptoms could predict mood symptoms, suicidal ideation and plans, and the cognitive component of hopelessness
“3) insomnia symptoms might mediate the effect of early life stressors on mood symptoms, hopelessness, and suicidal ideation and behaviors.”
Palagini suggested that “Insomnia symptoms should be easily addressed in clinical practice with 1–2 questions. Insomnia treatment should be considered as a treatment to prevent …relapse and recurrence [of bipolar disorder] and to prevent suicide and the effect of early life stress on [bipolar disorder].”
Editor’s Note: Regular nightly rating of mood, functioning, hours of sleep, medications, life events, side effects, and other comorbid symptoms on the Monthly Mood Chart Personal Calendar (pdf) is an easy way for patients with bipolar disorder to carefully track their illness trajectory and the completeness of their response to medications.
A decrease in the hours of sleep should be used as a possible early warning sign of impending difficulties, or even a new episode. Patients should discuss with their physician the threshold of insomnia (such as the loss of 2 hours of sleep for two days in a row) that should trigger a call to the physician, and what interventions the patient might initiate for lesser amounts of sleep loss and/or changes in mood. Heading these off early may prevent the breakthrough of a full-blown manic or depressive episode.
Lithium Corrects Circadian Rhythm Abnormalities in Bipolar Depression

At a recent scientific meeting, researcher Monica Federoff described new findings about lithium’s effects in people with bipolar I disorder, especially regarding circadian rhythms. The 12-week study included 386 participants with bipolar I. Some participants responded well to lithium, but even those whose bipolar disorder did not remit saw improvements in total symptoms, depressive symptoms, and manic symptoms.
Only those who were classified as good responders to lithium treatment showed improvement in circadian symptoms. Their depression improved in the direction of more “morningness,” and the authors suggested that “stabilization of circadian symptoms of depression may be an essential feature of lithium’s therapeutic effects in [bipolar] I patients.”
