
FDA Approves Extended-Release Aripiprazole Injected Monthly to Prevent Manic and Mixed Episodes in Bipolar I
In 2017 the US Food and Drug Administration approved a monthly injectable form of the atypical antipsychotic drug aripiprazole, Abilify Maintena, for the prevention of manic and mixed episodes in bipolar I disorder. The intramuscular injections are available for monotherapy in preparations of 300 mg or 400 mg. Maintena did not prevent depressive episodes.
Maintena is already FDA-approved for the treatment of schizophrenia and Tourette’s syndrome in adults.
The approval for bipolar I disorder follows a 52-week phase 3, double-blind, placebo-controlled randomized trial. Participants were experiencing a manic episode during screening for the study, met the criteria for bipolar I disorder, and had had at least one prior manic or mixed episode severe enough to require treatment.
Compared to placebo, Maintena in once-a-month injections delayed the recurrence of any mood episode following the initial manic episode at screening. When the researchers separated their analysis based on type of episode, Maintena reduced manic and mixed episodes compared to placebo, but did not do a better job than placebo at preventing depressive episodes.
An oral antipsychotic must be administered for 14 days following the first injection of Maintena. The extended-release injection is available as 300 mg– or 400 mg–strength powder that may be reconstituted, or as prefilled syringes.
Editor’s Note: Because Maintena is delivered as a once-a-month injection, it may be helpful for patients who struggle to take daily oral medications.
Midday Bright Light Therapy Improved Bipolar Depression

A study by Dorothy K. Sit and colleagues published in the American Journal of Psychiatry in 2017 found that delivering bright white light therapy to patients with bipolar depression between the hours of noon and 2:30pm improved their depression compared to delivering inactive dim light, and did not cause mood switches into mania. The study included 46 patients with moderate bipolar depression, no hypomania and no psychosis.
The active therapy group was exposed to broad-spectrum bright white fluorescent light at 7,000 Lux while the inactive group received dim red light at 50 Lux. Both groups were instructed to sit 12 inches from the light and face it without looking directly at it. The therapy began with 15-minute afternoon sessions and increased to 60 minutes per day by 4 weeks. Participants were assessed weekly. Remission rates increased dramatically in the active group beginning in the fourth week. At weeks 4 through 6, the remission rate for those in the active bright light group was 68.2% compared to only 22.2% in the dim light group.
Mean depression scores were better in the treated group, as were global functioning and response rates.
Some participants were taking antidepressants concurrently, and these participants were evenly distributed across the two study groups.
An earlier pilot study by the same researchers had found that bright light therapy delivered in the morning was followed by some hypomanic reactions or bipolar cycling. The midday sessions did not cause any mood switching.
Bright light therapy is often used to treat seasonal affective disorder (SAD) using a 10,000 Lux light box. This study took place mostly during the fall and winter months.
Editor’s Note: Bright light therapy is generally safe and boasts a high remission rate. Light boxes can be acquired without a prescription and are portable and easy to use. Midday light may have the best results and the least risk of provoking a mood switch into mania.
Making Lithium Treatment More Tolerable For Patients
 In a slideshow at Psychiatric Times, Chris Aiken describes seven ways to improve lithium’s tolerability. Since many researchers, including BNN Editor-in-Chief Robert M. Post, have suggested that lithium should be used more often as a treatment for bipolar disorder, ways of making its side effects more manageable are of great interest. Here we summarize Dr. Aiken’s seven points and add a few perspectives of our own.
In a slideshow at Psychiatric Times, Chris Aiken describes seven ways to improve lithium’s tolerability. Since many researchers, including BNN Editor-in-Chief Robert M. Post, have suggested that lithium should be used more often as a treatment for bipolar disorder, ways of making its side effects more manageable are of great interest. Here we summarize Dr. Aiken’s seven points and add a few perspectives of our own.
Aiken writes that “when it comes to the side effects that matter most to patients—sedation, weight gain, and cognition—lithium’s tolerability ranks right behind lamotrigine.” In fact, lithium plus lamotrigine is an excellent combination, as lithium excels at preventing manias while lamotrigine excels at depression prevention.
Post’s philosophy is that many of lithium’s side effects can be avoided in the first place through judicious dose titration. He suggests gradually increasing dosage, and stopping before side effects become difficult, or reducing a dosage that has already become a problem. The idea is to avoid lithium side effects even if blood levels of lithium remain below clinically therapeutic levels. Post suggests using lithium at whatever dose is not associated with side effects.
Many of lithium’s positive therapeutic effects emerge at low doses, and if this improvement is insufficient, the rest of the needed efficacy can be achieved by adding other medications. As noted above, lamotrigine is a good option for break-through depression, as is lurasidone. For breakthrough mania, the mood stabilizers valproate and carbamazepine or an atypical antipsychotic can be added to lithium.
A little-appreciated option for enhancing lithium’s mood stabilizing effects is nimodipine, a dihydropyridine calcium blocker. It has both antimanic and antidepressant efficacy without lithium’s side effects. Research showed that a year on the combination of lithium and nimodipine was more effective than a year of either drug alone.
If a patient taking lithium experiences a tremor at a dose that is not fully effective, nimodipine can be added in order to lower the lithium dose enough to eliminate the tremor.
Nimodipine specifically blocks the calcium influx gene CACNA1C that has been repeatedly been associated with the vulnerability to bipolar disorder and depression.
If side effects do occur on lithium, they can often be managed. The following suggestions are adapted from Aiken’s article with input from Post. Read more
The New News About Lithium
Robert M. Post, Editor-in-Chief of the BNN, recently published an open access article in the journal Neuropsychopharmacology, “The New News About Lithium: An Underutilized Treatment in the United States.” Here we summarize the main points of the publication, including: the multiple benefits of lithium, its relative safety, predictors of lithium responsiveness, and principles for treatment.
Benefits of lithium
Lithium prevents both depressions and manias in bipolar disorder, and also prevents depressions in unipolar disorder and can augment antidepressant effects acutely. In addition to these mood benefits, lithium has anti-suicide effects. Lithium also enhances the efficacy of atypical antipsychotics and other mood stabilizers when used in combination with them.
Lithium is good for the brain. It has been shown to reduce the incidence of dementia. Lithium increases the volume of the hippocampus and cortex, and can increase the production of new neurons and glia. It also protects neurons. In animals, lithium has been shown to reduce lesion size in neurological syndromes that are models for human disorders such as AIDS-related neurotoxicity, ischemic/hemorrhagic stroke, traumatic brain/spinal cord injury, Huntington’s disease, Alzheimer’s disease, amyotrophic lateral sclerosis (ALS or Lou Gehrig’s disease), fragile X syndrome, Parkinson’s disease, retinal degeneration, multiple sclerosis, alcohol-induced degeneration, Down’s syndrome, spinocerebellar ataxia-1, and irradiation.
Lithium’s benefits include more general ones as well. It can increase the length of telomeres, bits of DNA on the ends of chromosomes that protect them during replication. Short telomeres have been linked to various illnesses and the aging process. Lithium also decreases the incidence of several medical illnesses and enhances survival.
Side Effects Are Often Benign, Treatable
Lithium side effects are more benign than many people think. Even low levels of lithium may be therapeutically sufficient. Read more
Three Experts’ Different Approaches to Treating PTSD in Veterans
 In the BNN we have previously described some experts’ preferred treatment algorithms for patients with treatment-resistant post-traumatic stress disorder (PTSD), which is often complicated by traumatic brain injury (TBI). In this article, we update and expand upon these expert views.
In the BNN we have previously described some experts’ preferred treatment algorithms for patients with treatment-resistant post-traumatic stress disorder (PTSD), which is often complicated by traumatic brain injury (TBI). In this article, we update and expand upon these expert views.
David Bakish has worked as Medical Director at the Ottawa Psychopharmacology Clinic and is a former professor of psychiatry at the University of Ottawa in Ottawa, Ontario. In addition, he works with the Canadian military seeing patients with PTSD, substance abuse, and traumatic brain injuries. He uses a symptom-driven approach to PTSD, including 6 to 7 targeted medications added in sequence.
Albert Sattin is a professor of psychiatry and biobehavioral sciences at UCLA, belongs to their Brain Research Institute, and is affiliated with both the Ronald Reagan UCLA Medical Center and the Veterans Affairs Greater Los Angeles Healthcare System. He prefers to treat PTSD with a three-part combination of the blood pressure–lowering drug prazosin, a selective serotonin reuptake inhibitor (SSRI) antidepressant, and the atypical antidepressant mirtazapine.
Murray Raskind pioneered placebo-controlled studies of prazosin for PTSD and served as director of the Veterans Affairs Puget Sound Health Care System Mental Health Service, in addition to serving in the Department of Psychiatry and Behavioral Sciences at the University of Washington School of Medicine. Raskind’s approach to PTSD includes prazosin, the tricyclic antidepressant amitriptyline, and if needed for sleep, the sedative zolpidem.
Only SSRIs are approved by the US Food and Drug Administration (FDA) for the treatment of PTSD, but these on their own are rarely sufficient to handle the insomnia and other symptoms that accompany PTSD. Exposure therapy, in which patients are gradually led to approach trauma-related memories, feelings, and situations they previously avoided, is the most recommended type of therapy, but it too is often insufficient to treat all the complexities of the illness. Read on for more on each doctor’s approach to treating PTSD. Read more
Deep TMS May Improve Treatment-Resistant Bipolar Depression
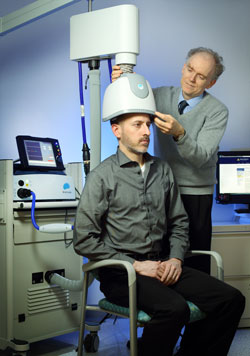 Deep transcranial magnetic stimulation (dTMS) is a non-invasive treatment that has been shown to be effective in unipolar depression. It consists of a helmet fitted to the head, which uses magnetic coils to create an electric field in a desired brain region.
Deep transcranial magnetic stimulation (dTMS) is a non-invasive treatment that has been shown to be effective in unipolar depression. It consists of a helmet fitted to the head, which uses magnetic coils to create an electric field in a desired brain region.
A 2017 double-blind randomized study by Diego F. Taveres and colleagues in the journal Neuropsychopharmacology found that 20 sessions of dTMS targeting the left dorsolateral prefrontal cortex produced greater improvement in bipolar depression over 4 weeks of treatment than the same number of sham sessions in which participants wore a helmet that delivered similar sounds and scalp sensations without the electrical effects to the brain. The participants had treatment-resistant bipolar depression that was being treated with medication.
However, dTMS’ effects were not significantly different from those of the sham over four additional weeks of follow-up, nor were remission rates significantly different across the two groups. Out of 50 participants, seven dropped out of the study—two from the sham group, and five from the active dTMS group. But there were no occasions on which a participant switched into mania following treatment.
This study suggests that dTMS has the potential to more rapidly improve treatment-resistant bipolar depression as well as unipolar depression.
Evidence-Based Psychotherapies for Young Children
 As many as 7–10% of children under the age of 5 have mood or behavioral problems, and this risk is even higher when a parent has a mood disorder. However, many families are not able to access treatment for these children due to their location, a lack of providers, or insurance problems.
As many as 7–10% of children under the age of 5 have mood or behavioral problems, and this risk is even higher when a parent has a mood disorder. However, many families are not able to access treatment for these children due to their location, a lack of providers, or insurance problems.
A 2016 article by Mary Margaret Gleason and colleagues in the journal Technical Report in Pediatrics summarizes psychotherapeutic treatments for children that are supported with rigorous evidence. Some of these include infant-parent psychotherapy, video feedback for positive parenting, attachment biobehavioral catch-up (or ABC, in which caregivers are taught to re-interpret the signals of children who previously experienced maltreatment, providing nurturing in response), parent-child interaction therapy, and programs that combine parenting support with illness prevention, such as the Incredible Years series (for behavioral difficulties), the New Forest Programme (for attention-deficit hyperactivity disorder or ADHD), and Helping the Noncompliant Child (for oppositional behavior).
Gleason and colleagues suggest that pediatricians should take the lead in assessing young children and recommending appropriate psychotherapeutic approaches.
One resource available to parents is our own Child Network. It consists of an online portal where parents can provide weekly ratings of their children’s symptoms. These can be provided to the child’s physician to facilitate diagnosis and to clinicians to more effectively evaluate the results of treatment. The data provided to the Child Network will in turn help us understand how children are being treated in the community. There a few initial forms to fill out, but the weekly rating process is quick and can provide a great picture of a child’s wellbeing over time, including evaluating the effectiveness of any treatments.
Generic Seroquel XR Approved
 Earlier this year, the US Food and Drug Administration approved a generic version of Seroquel XR tablets (Quetiapine Fumarate Extended-Release Tablets), which are used to treat both depression and mania in bipolar disorder, schizophrenia, and to augment the effects of antidepressants in unipolar depression. Also known as quetiapine, the generic tablets will be available in 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg doses.
Earlier this year, the US Food and Drug Administration approved a generic version of Seroquel XR tablets (Quetiapine Fumarate Extended-Release Tablets), which are used to treat both depression and mania in bipolar disorder, schizophrenia, and to augment the effects of antidepressants in unipolar depression. Also known as quetiapine, the generic tablets will be available in 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg doses.
Seroquel XR is taken once per day several hours before bedtime in the acute treatment for bipolar depression (300 mg/day), mania or mixed episodes (300–600 mg/day) or their prevention (400 mg/day); or paired with antidepressants to treat unipolar depression (150–300 mg/day).
The generic tablets, which are expected to be more affordable than Seroquel XR, are produced by Pharmadax Inc.
Some Antacids Cause Kidney Damage with No Prior Symptoms
 Commonly used antacids such as Prevacid, Nexium, Prilosec, and Protonix can impair kidney function, according to a 2017 article in the journal Kidney International. These drugs, known as proton pump inhibitors or PPIs, should not be taken long-term without monitoring of kidney function. Other antacids that work by blocking histamine H2 receptors do not interfere with kidney function but may not work as well as PPIs.
Commonly used antacids such as Prevacid, Nexium, Prilosec, and Protonix can impair kidney function, according to a 2017 article in the journal Kidney International. These drugs, known as proton pump inhibitors or PPIs, should not be taken long-term without monitoring of kidney function. Other antacids that work by blocking histamine H2 receptors do not interfere with kidney function but may not work as well as PPIs.
Researcher Yan Xie and colleagues found that more than half of people who developed chronic kidney damage while taking PPIs showed no earlier acute signs of kidney dysfunction, meaning there may not be signs of kidney function loss until the damage is irreversible. Xie and colleagues suggest that patients and doctors should be more vigilant about monitoring the use of these medications, since waiting for outward signs of declining kidney function is not a reliable way of detecting damage.
More than 15 million Americans use prescription PPIs to reduce gastric acid, bringing relief to heartburn, ulcers, and acid reflux. Millions more buy PPIs over the counter without consulting a doctor about their use.
The study analyzed Department of Veterans Affairs data from 125,596 new users of PPIs and 18,436 new users of H2 blockers. Acute, reversible symptoms of kidney damage, such as reduction in the urine being cleared from the body, fatigue, and swelling of the legs and ankles were seen in less than 20% of the PPI users. However, more than half of those who developed chronic kidney damage and end-stage renal disease never showed these warning signals beforehand. In contrast, only 7.67% of those taking H2 blockers had chronic kidney disease without acute symptoms, and 1.27% had end-stage renal disease, when kidneys can no longer clear waste from the body, and dialysis or a kidney transplant is required.
Xie and colleagues suggest carefully monitoring kidney function in people taking PPIs, even when there are no outward signs of problems. They also suggest carefully evaluating whether PPIs are necessary, since the risk of kidney damage is serious.
Methylphenidate Does Not Cause Mania When Taken with a Mood Stabilizer
 Methylphenidate is an effective treatment for attention-deficit hyperactivity disorder (ADHD). Ritalin may be the most commonly recognized trade name for methylphenidate, but it is also sold under the names Concerta, Daytrana, Methylin, and Aptensio. A 2016 article in the American Journal of Psychiatry reports that methylphenidate can safely be taken by people with bipolar disorder and comorbid ADHD as long as it is paired with mood-stabilizing treatment.
Methylphenidate is an effective treatment for attention-deficit hyperactivity disorder (ADHD). Ritalin may be the most commonly recognized trade name for methylphenidate, but it is also sold under the names Concerta, Daytrana, Methylin, and Aptensio. A 2016 article in the American Journal of Psychiatry reports that methylphenidate can safely be taken by people with bipolar disorder and comorbid ADHD as long as it is paired with mood-stabilizing treatment.
The study was based on data from a Swedish national registry. Researchers led by Alexander Viktorin identified 2,307 adults with bipolar disorder who began taking methylphenidate between 2006 and 2014. Of these, 1,103 were taking mood stabilizers including antipsychotic medications, lithium, or valproate, while 718 were not taking any mood stabilizing medications.
Among those who began taking methylphenidate without mood stabilizers, manic episodes increased over the next six months. In contrast, patients taking mood stabilizers had their risk of mania decrease after beginning treatment with methylphenidate.
Viktorin and colleagues suggest that 20% of patients with bipolar disorder may also have ADHD, so it is not surprising that 8% of patients with bipolar disorder in Sweden receive a methylphenidate prescription.
Mood-stabilizing drugs can worsen attention and concentration, so methylphenidate treatment can be helpful if it can be done without increasing manic episodes. However, Viktorin and colleagues suggest that due to the risk of increasing mania, anyone given a prescription for methylphenidate monotherapy should be carefully screened to rule out bipolar disorder.
The researchers confirmed that taking methylphenidate for ADHD while taking a mood stabilizer for bipolar disorder is a safe combination.
