
Depression and Bipolar Disorder in Adolescence Linked to Early-Onset Cardiovascular Disease and Hardening of the Arteries
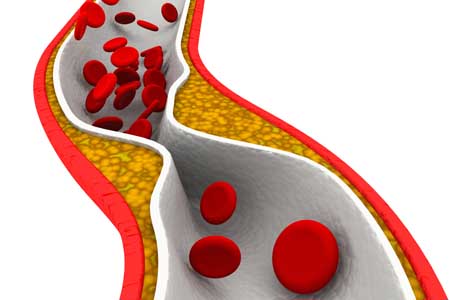
The link between mood disorders and cardiovascular illnesses has been clear for some time. Now there is evidence that this link begins early in life. In 2015, the American Heart Association issued a statement that adolescents with major depressive disorder and bipolar disorder are at increased risk for both accelerated atherosclerosis (narrowing and hardening of the arteries) and early-onset cardiovascular disease.
In the statement, the American Heart Association recommended that major depressive disorder and bipolar disorder be classified as “tier II” conditions (which also include HIV and chronic inflammatory disease) that confer a moderate risk of disease.
Until recently, it had been assumed that the increased risk of cardiovascular disease among people with depression or bipolar disorder was a result of behaviors linked to these illnesses, such as higher rates of smoking, obesity, or diabetes, which increases heart disease. Some psychiatric medication can also bring about risk factors for cardiovascular problems. It turns out that these types of factors could not fully explain the increased risk of atherosclerosis and cardiovascular disease among people who had depression or bipolar disorder in their teens.
It is not clear why depression and bipolar disorder make cardiovascular illness more likely, though it may be due to blood vessel damage resulting from inflammation or oxidative stress.
The American Heart Association recommends that pediatricians and cardiologists pay particular attention to this link by identifying and treating mental illness as early as possible and by making sure that their colleagues understand the role of mental illnesses in cardiovascular risk.
Anxiety, Depression, Unstable Mood, and Low-Level Mania Best Predictors of Bipolar Disorder

Researchers are looking for better ways of predicting whether children at risk for bipolar disorder will go on to develop the illness. A 2015 study by David Axelson and colleagues in the American Journal of Psychiatry reported that in the offspring of parents with bipolar disorder, diagnoses of sub-threshold mania, depression, and disruptive behavior disorders were associated with subsequent diagnosis of full-blown Bipolar I or Bipolar II disorders six to seven years later.
More recently, in an article by Danella M. Hafeman and colleagues in the American Journal of Psychiatry, the same group of investigators has examined how symptoms (rather than categorical diagnoses, as in the earlier study) predict the development of bipolar disorder. In children and adolescents at high risk for bipolar disorder (because they have a parent with the disorder) three types of symptoms were the best predictors of later bipolar disorder: anxiety/depression at the time participants entered the study, unstable mood or irritability both when entering the study and shortly before a bipolar diagnosis, and low-level manic symptoms observed shortly before diagnosis.
The earlier the age at which a parent was diagnosed with a mood disorder, the greater the risk that the offspring would also be diagnosed with bipolar disorder. Youth with all four risk factors (anxiety or depression, mood changes, low-level mania, and a parent who was diagnosed with a mood disorder at an early age) had a 49 percent chance of developing bipolar disorder, compared to a 2 percent chance among those without those risk factors.
Childhood onset of bipolar disorder and long delays until first treatment for depression or mania are both significant predictors of a poor outcome in adulthood compared to adult onsets and shorter delays to treatment. Read more
Psychotherapy Improves Outcomes for People with Bipolar Disorder

Studies have shown that therapy can be helpful for people with bipolar disorder. In a 2016 article in the British Journal of Psychiatry, researchers led by M. Oud described the findings of their systematic review of studies evaluating different types of therapy for bipolar disorder. The research team reviewed the findings of 55 randomized controlled trials of psychotherapeutic interventions that included a total of 6,010 adult participants with bipolar disorder. The team found moderate-quality evidence that psychological interventions reduced relapses following treatment, and that collaborative care reduced hospital admissions for adults with bipolar disorder. Oud and colleagues found lower-quality evidence that group interventions reduced depression relapses following treatment, and that family psychoeducation reduced symptoms of depression and mania.
The reseachers concluded that there is evidence that therapy can be helpful for people with bipolar disorder. Since some of the evidence was of low quality, more research is needed to identify the most effective therapies for different phases of bipolar disorder.
Editor’s Note: The data are clear that therapy is helpful. In particular, one approach worth emulating is that described in an article by Lars V. Kessing and colleagues in the British Journal of Psychiatry in 2013. They found that comprehensive care in an outpatient mood disorder clinic, which included psychotherapy, psychoeducation, mood monitoring, and drug treatment, reduced relapses significantly compared to treatment as usual.
Inflammation Linked to Bipolar Illness in Young People
 The Course and Outcome of Bipolar Youth study, or COBY, has been collecting information on young people with bipolar disorder and tracking their symptoms into adulthood since 2000. A 2015 study by Benjamin I. Golstein in the Journal of Clinical Psychiatry analyzed COBY data, identifying links between higher than average levels of inflammatory markers measured in the blood and participants’ histories of illness and familial risk factors.
The Course and Outcome of Bipolar Youth study, or COBY, has been collecting information on young people with bipolar disorder and tracking their symptoms into adulthood since 2000. A 2015 study by Benjamin I. Golstein in the Journal of Clinical Psychiatry analyzed COBY data, identifying links between higher than average levels of inflammatory markers measured in the blood and participants’ histories of illness and familial risk factors.
High levels of the inflammatory marker hsCRP were associated with longer duration of illness, substance use disorder, and family history of suicide attempts or completed suicides. High levels of TNF-alpha were linked to suicide attempts, self-injury behaviors, and family history of substance use disorders. IL-6 was also linked to family history of substance use disorders.
There were also links between inflammatory markers and participants’ symptoms over the 6 months leading up to the blood tests. Levels of the inflammatory marker TNF-alpha were linked to the percentage of weeks patients had psychotic symptoms. Levels of IL-6 were associated with percentage of weeks with subthreshold mood symptoms and also with any suicide attempt. Levels of HsCRP were linked to maximum severity of depressive symptoms.
It is possible that targeting the elevated levels of inflammatory markers with anti-inflammatory treatments could improve patients’ response to treatments, but this topic requires further study.
Facial Emotion Recognition Deficient in Bipolar Disorder
![]()
In the past decade, several studies have indicated that people with bipolar disorder have less ability to recognize the emotions expressed on people’s faces than do healthy controls. A 2013 meta-analysis by Cecilia Samamé and colleagues concluded that facial emotion recognition was deficient in people with bipolar disorder regardless of their current state. A 2011 quantitative review article by Christian G. Kohler and colleagues revealed that this difficulty distinguishing emotions is general, rather than specific to any one emotion.
A 2015 study by Esther Vierck and colleagues in the journal Psychiatry Research showed that both euthymic patients with bipolar disorder and their first-degree relatives without bipolar disorder performed worse on tests of emotion recognition than did normal controls. The findings in healthy relatives suggest that the deficit may be a familial risk factor for the development of bipolar disorder.
These deficits in facial emotion recognition have also been seen in 4 out of 5 studies of children with early-onset bipolar disorder, including those who are euthymic. 2008 studies by Melissa A. Brotman and colleagues showed that even children just at high risk for bipolar disorder due to a family history of the disorder had deficient emotion recognition.
This literature indicates that deficiencies in facial emotion recognition consistently accompany bipolar disorder and may also be a sign that a child or teenager is at risk for bipolar disorder. Since these deficits can create social and interpersonal difficulties, it may be useful to teach better emotion recognition skills to people with bipolar disorder or those at high risk for the illness.
Antioxidant NAC Improves Symptoms of Schizophrenia and Bipolar Disorder

N-acetylcysteine (NAC), an antioxidant available without a prescription in health food stores, has shown remarkable effectiveness when added to regular treatments for schizophrenia, bipolar disorder, and the substance abuse that often accompanies these illnesses.
A 2008 article by Michael Berk and colleagues in the journal Biological Psychiatry reported that compared to placebo, 2 grams/day of NAC reduced both positive symptoms of schizophrenia (hallucinations, delusions) and negative symptoms (social withdrawal, difficulty planning and problem-solving). A 2013 study by Mehdi Farokhnia found that 2 grams/day of NAC improved negative symptoms in 42 patients with schizophrenia. Two other studies found that NAC improved deficits in auditory sensory processing in people with schizophrenia.
NAC also improves symptoms of bipolar disorder. A 2008 study by Berk and a 2011 study by Pedro Vieira da Silva Magalhães showed that NAC improved bipolar depression, and a small 2013 study by Magalhães showed that it improved mania in 15 patients. After 24 weeks, 60% of those who took NAC were in remission, compared to 15% of those taking placebo.
NAC is also effective at reducing habitual behaviors such as substance abuse, which is common in patients with schizophrenia and bipolar disorder. Studies have shown that NAC can reduce patients’ use of marijuana, cocaine, alcohol, and nicotine. It is relatively safe with minimal side effects, and fights oxidative stress, which is also common in severe mental illness.
NAC comes in 500mg or 600mg capsules. Dosing typically begins with one capsule twice a day for a week, followed by two tablets twice a day thereafter. As with any recommendations in the BNN, these should not be acted on without guidance from a treating physician.
Stem Cell Research May Help Explain Biochemistry of Bipolar Disorder
At the 2015 meeting of the International Society for Bipolar Disorders, researcher Martin McInnis described how stem cells can be used to identify biochemical abnormalities in patients with bipolar disorder. In this research, the stem cells, or IPSCs (for induced pluripotential stem cells), are created when cells from skin fibroblasts, which produce connective tissue, are treated with chemicals that cause them to de-differentiate back into stem cells.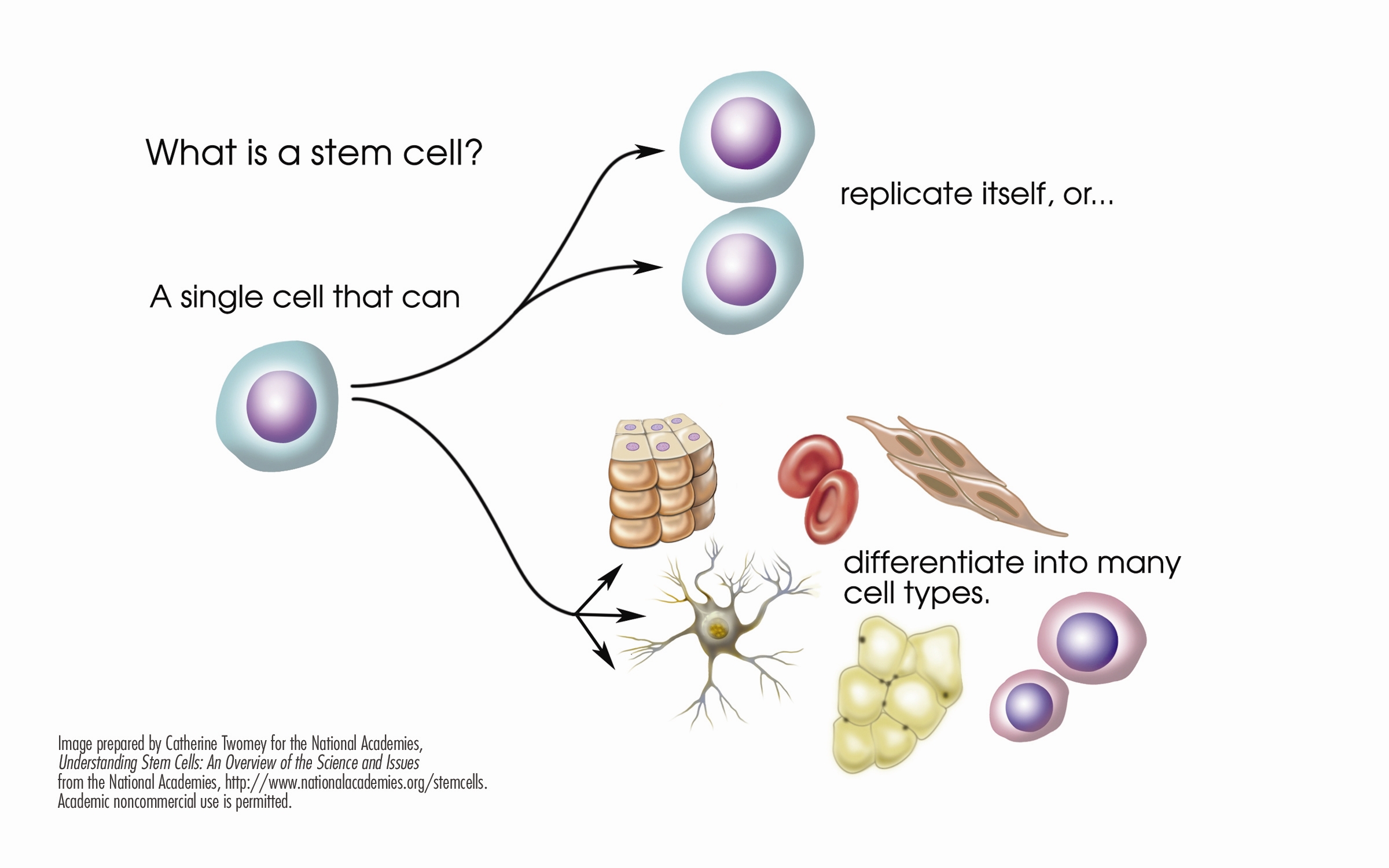
McInnis identified several abnormalities in the stem cells of patients with bipolar disorder. Stem cells with the gene CACNA1C, which is associated with vulnerability to bipolar disorder, fired more rapidly than non-CACNA1C stem cells. There were other abnormalities at the NMDA glutamate receptor and an imbalance of the neurotransmitter GABA in the cells. When the cells were treated with lithium, some of these abnormalities were reversed. In the cells with the CACNA1C gene, lithium normalized the firing rate. Lithium aslo re-balanced the distribution of GABA in the cells.
McInnis hopes that this stem cell research will shed light on the abnormalities associated with bipolar disorder, help explain how lithium corrects some of these, and lead to the development of new therapeutic approaches.
Reduced Cognitive Function and Other Abnormalities in Pediatric Bipolar Disorder
 At the 2015 meeting of the International Society for Bipolar Disorders, Ben Goldstein described a study of cognitive dysfunction in pediatric bipolar disorder. Children with bipolar disorder were three years behind in executive functioning (which covers abilities such as planning and problem-solving) and verbal memory.
At the 2015 meeting of the International Society for Bipolar Disorders, Ben Goldstein described a study of cognitive dysfunction in pediatric bipolar disorder. Children with bipolar disorder were three years behind in executive functioning (which covers abilities such as planning and problem-solving) and verbal memory.
There were other abnormalities. Youth with bipolar disorder had smaller amygdalas, and those with larger amygdalas recovered better. Perception of facial emotion was another area of weakness for children (and adults) with bipolar disorder. Studies show increased activity of the amygdala during facial emotion recognition tasks.
Goldstein reported that nine studies show that youth with bipolar disorder have reduced white matter integrity. This has also been observed in their relatives without bipolar disorder, suggesting that it is a sign of vulnerability to bipolar illness. This could identify children who could benefit from preemptive treatment because they are at high risk for developing bipolar disorder due to a family history of the illness.
There are some indications of increased inflammation in pediatric bipolar disorder. CRP, a protein that is a marker of inflammation, is elevated to a level equivalent to those in kids with juvenile rheumatoid arthritis before treatment (about 3 mg/L). CRP levels may be able to predict onset of depression or mania in those with minor symptoms, and is also associated with depression duration and severity. Goldstein reported that TNF-alpha, another inflammatory marker, may be elevated in children with psychosis.
Goldstein noted a study by Ghanshyam Pandey that showed that improvement in pediatric bipolar disorder was related to increases in BDNF, a protein that protects neurons. Cognitive flexibility interacted with CRP and BDNF—those with low BDNF had more cognitive impairment as their CRP increased than did those with high BDNF.
Treating Bipolar Disorder in Children and Adolescents

Bipolar disorder in childhood or adolescence can destroy academic, family, and peer relationships and increase vulnerability to drug use, unsafe sexual encounters, disability, and suicide. Treatment is critical to avoid cognitive decline. Given the potential tragic outcomes of undertreating bipolar illness, it is concerning that 40–60% of children and adolescents with bipolar disorder are not in treatment.
In a talk at the 2015 meeting of the International Society for Bipolar Disorder, researcher Cristian Zeni reviewed the existing research on the treatment of bipolar disorder in children and adolescents. A 2012 study by Geller reported response rates of 68% for the atypical antipsychotic risperidone, 35% for lithium and 24% for valproate. Risperidone was linked to weight gain and increases in prolactin, a protein secreted by the pituitary gland, while lithium was linked to more discontinuations and valproate to sedation.
For children or adolescents with aggression, researcher Robert Kowatch recommends quetiapine, aripiprazole, and risperidone. For those with a family history of bipolar disorder, he recommends lithium or alternatively, valproate plus an atypical antipsychotic.
Reseacher Robert Findling has found that lamotrigine has positive effects in childhood mania, and Duffy et al. found in a study of 21 children with mania that 13 remained stable on monotherapy with quetiapine for 40 weeks without relapse, while 5 others required combination treatment with more than one drug. In studies by Karen Wagner, oxcarbazepine was significantly better than placebo at reducing mania in younger children (ages 7–12), but not older children (13–18).
Studies by Duffy and colleagues in 2007 and 2009 recommend lithium for those with a family history of bipolar disorder, atypical antipsychotics for children with no family history of bipolar disorder, and lamotrigine for those with a family history of anxiety disorders.
In children with bipolar disorder and comorbid attention deficit hyperactivity disorder, there is universal agreement that mood should be stabilized first, and then small amounts of stimulants may be added for residual ADHD symptoms. Too often, the opposite occurs, with stimulants given prior to mood stabilization with lithium, anticonvulsants (valproate, lamotrigine, carbamazepine/oxcarbazepine) and/or an atypical antipsychotic. Read more
Predictors of Bipolar Disorder in At-Risk Youth

A new longitudinal study of 391 youth at risk for bipolar disorder revealed some predictors of the disorder. The study by Danella M. Hafeman and colleagues was presented at the 2015 meeting of the Society of Biological Psychiatry. The participants were aged 6–18 and each had a parent with bipolar disorder. Over the course of the study, 40 developed an illness on the bipolar spectrum, including 21 who developed bipolar I or II. The participants were assessed for various descriptive characteristics and those who developed bipolar disorder were compared to those who developed major depressive disorder.
The most important predictors of bipolar disorder were parental assessment of internalizing symptoms of anxiety or depression, self-assessment of mood changeability, and self-assessment of hostility. A diagnosis of bipolar disorder not otherwise specified (BP-NOS) was the only predictor of a later diagnosis of bipolar I or II.
Editors Note: These data resemble findings from a 2015 study by David Axelson and colleagues in the American Journal of Psychiatry that used the same cohort of participants. The Axelson study indicated that a categorical diagnosis of a major psychiatric disorder occurred in 74% of the offspring of a bipolar parent compared to about 50% in a control group from the community. Depression, anxiety, attention deficit hyperactivity disorder (ADHD), and oppositional disorders were even more common than bipolar disorder in the at-risk population.
The presence of a major psychiatric diagnosis in about three-quarters of the offspring of a parent with bipolar disorder suggests the importance of early vigilance. One way to track symptoms of depression, anxiety, ADHD, oppositional behavior, and bipolar disorder is to join the Child Network, a secure online platform for rating children’s moods, medications, and side effects. These weekly ratings can be collected longitudinally and printed out to help parents and clinicians assess mood difficulties in their children.
