
An Inflammatory State Impedes Treatment for Bipolar Disorder
 A 2017 study by in the Journal of Clinical Psychiatry links inflammation to a poor antidepressant response in bipolar disorder. Many previous studies have found that elevated inflammatory markers are common in mood disorders, and that an inflammatory state seems to prevent response to certain therapies.
A 2017 study by in the Journal of Clinical Psychiatry links inflammation to a poor antidepressant response in bipolar disorder. Many previous studies have found that elevated inflammatory markers are common in mood disorders, and that an inflammatory state seems to prevent response to certain therapies.
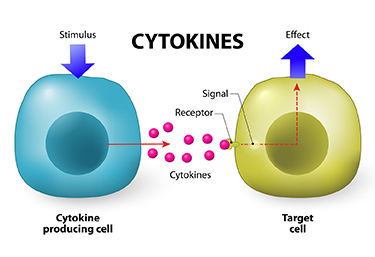
Researcher Francesco Benedetti and colleagues report that high levels of inflammatory cytokines (a type of small proteins) predicted a worse response to treatment with sleep deprivation and light therapy for bipolar depression. This treatment typically brings about a rapid antidepressant response.
Benedetti and colleagues measured 15 immune-regulating compounds in 37 patients who were experiencing an episode of bipolar depression and 24 healthy volunteers. Among those participants with bipolar disorder, 84% had a history of non-response to medication. Twenty-three of the 37 patients, or 62%, responded to the sleep deprivation/light therapy combination. Those who did not had higher levels of five cytokines: interleukin-8, monocyte chemoattractant protein-1, interferon-gamma, interleukin-6, and tumor necrosis factor-alpha.
Body mass index was correlated with cytokine levels and also reduced response to the treatment.
The finding supports a link between the immune system and mood disorders. Evaluating a patient’s level of inflammation may, in the future, allow doctors to predict the patient’s response to a given therapy. Patients with high levels of inflammation might benefit most from treatments that target their immune system.
A Calculator of Risk for Bipolar Disorder in Youth
Daniella Hafeman of the University of Pittsburgh described a risk calculator for predicting an individual’s risk for bipolar disorder, which is available at www.pediatricbipolar.pitt.edu. Possible factors included in the risk calculation include a parent’s early age of onset of bipolar disorder, mood shifts early in life, a child’s anxiety or depression symptoms, later affective mood shifts, and new onset of subthreshold mania.
Editor’s Note: A “poor man’s” assessment of risk can also be of help to a family or clinician. There are four components. The first is genetic. Having one parent with bipolar disorder is a potent risk factor, and can be further magnified if the other parent also has a mood disorder. If three or more first degree relatives or three or more generations of first degree relatives have a mood disorder, this further increases risk four- to six-fold.
Perinatal vulnerability is another factor. Beyond these genetic vulnerabilities, a history of maternal toxoplasmosis or a viral infection during pregnancy, or the infant being noticeably underweight at birth can contribute to bipolar risk.
Childhood adversity also contributes to vulnerability to early onset of bipolar illness. A history of psychosocial stress in the child’s early years, such as abuse or abandonment, can be an added risk factor.
Prodromal or preliminary symptoms are also a risk factor. The development of an anxiety or depressive disorder, a disruptive behavioral disorder, or a bipolar not-otherwise-specified diagnosis (BP-NOS, used to describe manic symptoms of short duration) further increases risk. In studies by David Axelson and Boris Birmaher, 50% of children with an initial diagnosis of BP-NOS developed full-blown bipolar I or II illness upon several years of followup if there was a family history of bipolar disorder. About one-third converted to full bipolar disorder if there was no family history of bipolar disorder.
Thus, if a child has three or all four types of risk factors, their risk would be substantial. In this case, one might consider attempts at prevention. This could include a good diet rich in omega-3 fatty acids, regular exercise, joining a school sports team, developing good sleep habits, playing a musical instrument, and engaging in something akin to family focused therapy. Family focused therapy emphasizes psychoeducation, good communication skills, and problem solving. Attending to and treating parents’ symptoms and building a support system for both parents and the child can also help.
While these endeavors are not a guarantee to prevent the onset of more severe illness, they are all health-promoting in general and have few downsides.
Expectations Can Affect Treatment Efficacy
 A 2017 article by Vanda Faria and colleagues in the journal EBioMedicine reports that when patients with social anxiety disorder were told they were being treated with an active drug, they had a response rate three times higher than patients who were given the same drug but told it was an inactive placebo. The researchers suggest that the way treatments are presented to patients affects whether they work.
A 2017 article by Vanda Faria and colleagues in the journal EBioMedicine reports that when patients with social anxiety disorder were told they were being treated with an active drug, they had a response rate three times higher than patients who were given the same drug but told it was an inactive placebo. The researchers suggest that the way treatments are presented to patients affects whether they work.
In the study by Faria and colleagues, patients with social anxiety were given the selective serotonin reuptake inhibitor (SSRI) antidepressant escitalopram for nine weeks. Some were told they had received escitalopram, while some were told they had received a placebo. Not only did those who were told they were taking escitalopram see greater reductions in their anxiety, they also showed more connectivity between the posterior cingulate and the amygdala, a region that is crucial to mediating anxiety.
This finding is in line with other research that has found that patients’ thoughts and expectations during treatment can affect the efficacy of that treatment.
Researcher Isaac Marks found that patients with obsessive compulsive disorder (OCD) with fear of contamination who were told to avoid things they feared, such as touching a toilet seat, did not fare any better than those taking placebo pills. However, those taking SSRIs who tried new behaviors like touching a toilet seat learned that they could do so without a major fear response, and their phobias improved.
Several studies have shown that expectations of antidepressant efficacy have a big effect on whether patients with unipolar depression improve after beginning treatment with SSRIs. Bret R. Rutherford and colleagues reviewed findings on expectancy in major depressive disorder in a 2010 article in the journal Current Psychiatry Review.
When patients are presented with a drug and encouraged to believe it will work, they may gain the confidence to try out new behaviors or ways of looking at things, whether that means exploring new social situations for someone with social anxiety, or feeling hopeful and breaking the habit of negative rumination for someone with depression. As the study by Faria and colleagues shows, expectations can even change patterns of brain connectivity.
Studies of repetitive transcranial magnetic stimulation (rTMS), in which electromagnets placed near the scalp stimulate electrical impulses in the brain, have shown that patients with depression who engage in positive thoughts and conversations with their rTMS provider during the stimulation improve more than those who sit passively. If a patient engages in their habitual negative ruminations during rTMS, these might even be cemented by the rTMS-induced release of glutamate and brain-derived neurotrophic factor (BDNF), which are both involved in learning and memory processes and what has been called experience-dependent neuroplasticity.
Thus, a patient’s thoughts and outlook during treatment may be important to the therapeutic outcomes achieved. While expectations may not be sufficient to produce an effect on their own, it does seem that thoughts and behaviors can improve a treatment’s efficacy.
A New Treatment for Disruptive Mood Dysregulation

The 2013 update to the Diagnostic and Statistical Manual of Mental Disorders, or the DSM-5, included a new diagnosis of disruptive mood dysregulation disorder. Children with persistent, severe temper outbursts and irritable or angry moods that are out of proportion to circumstances may be diagnosed with the disorder. However, there is not much specificity to the diagnosis and few treatment studies have been done to help clinicians and parents determine how to manage symptoms of the disorder.
A poster presented at the 2017 Psych Congress reported that a medication protocol consisting of an anticonvulsant drug to stabilize moods and temper outbursts and a dopamine agonist to reduce irritability, impulsivity, and concentration problems reduced rates of re-hospitalization. The retrospective study by researchers D. Matthews and G. Matthews included 91 children and adolescents who were prescribed the anticonvulsant oxcarbazepine and the dopamine agonist amantadine following hospitalization for severe aggression, mood instability, and impulsivity. Those who stuck to the regimen with minimal changes for one year had an 8% re-hospitalization rate compared to a 26% re-hospitalization rate among those who discontinued the regimen or substituted other drugs.
Editor’s Note: Oxcarbazepine has a long-acting preparation, Oxtellar, that can be given all at night.
Amantadine (Symmetrel) not only is a dopamine agonist used for Parkinson’s disease, but is also an antiviral and a blocker of glutamate NMDA channels. It stabilizes the closed state of the NMDA channel.
Even Light Exercise Prevents Future Depressions

A 2017 article in The American Journal of Psychiatry suggests that regular leisure-time exercise of any intensity can protect against future depressions.
The study by Samuel B. Harvey and colleagues followed a group of 33,908 healthy adults for 11 years. The researchers found a link between regular leisure-time exercise and reduced incidence of future depression (but not anxiety). This link occurred regardless of the intensity of the exercise, and most of the effect occurred at low levels of exercise. Analysis suggested that 12% of future cases of depression could be prevented if all participants fit one hour of physical activity into their week.
A small part of the benefit came from the social and physical health benefits of exercise.
Harvey and colleagues suggested that from a public health perspective, increasing population levels of exercise modestly could lead to a substantial decrease in depressions.
Editor’s Note: Alongside maintenance treatment, in the form of antidepressants for unipolar depression or mood stabilizers and atypical antipsychotics for bipolar disorder, exercise could provide some benefits in preventing future depressions.
Simvastatin Looks Promising in Treatment of Negative Symptoms of Schizophrenia

The statin drug simvastatin (Zocor) enhances the effects of risperidone on negative symptoms of schizophrenia, according to a 2017 article by Soode Tajik-Esmaeeli and colleagues in the journal International Clinical Psychopharmacology.
In the 8-week study, 40 mg/day of simvastatin enhanced the effects of 4–6 mg/day of the antipsychotic risperidone on negative symptoms of schizophrenia, such as apathy and withdrawal, but not positive symptoms such as hallucinations or delusions.
Other statins, lovastatin and pravastatin, have not had a similar effect, possibly because they do not cross the blood-brain barrier as easily as simvastatin does.
Simvastatin has other benefits as well. Like all statins it decreases lipid levels, reducing cardiovascular disease. People with schizophrenia and bipolar disorder are at especially high risk for cardiovascular disease.
Simvastatin also decreases inflammation (lowering IL-1 alpha and TNF-beta levels) and may be neuroprotective, as it increases brain-derived neurotrophic factor (BDNF), a protein that protects neurons and is important for learning and memory. Inflammation is increasingly implicated in schizophrenia and bipolar disorder.
There is also some evidence that statins can prevent depressions over long-term follow-up. Studies in women without depression and men who had recently had heart attacks both showed that those taking statins had a lower rate of future depression than those not taking statins.
Editor’s Note: These findings suggest a potential 5-fold benefit to simvastatin: 1) It reduces negative symptoms in schizophrenia. 2) It reduces inflammation. 3) It increases BDNF. 4) It decreases cardiovascular disease risk by lowering lipid levels. 5) It may prevent future depressions.
Other approaches to augmenting schizophrenia treatment include nutritional supplements vitamin D3 and folate. Patients with psychosis often have vitamin D deficits. Folate supplements can reduce homocysteine, which has been linked to cognitive deficits in schizophrenia.
Liraglutide Decreased Body Weight, Improved Glucose Tolerance and Cardio Health in Schizophrenia
 A 2017 article by Julie R. Larsen and colleagues in the journal Archives of General Psychiatry reported that the drug liraglutide, a treatment for type 2 diabetes, improved certain health measures in people with schizophrenia who were overweight and prediabetic and being treated with the atypical antipsychotics olanzepine or clozapine.
A 2017 article by Julie R. Larsen and colleagues in the journal Archives of General Psychiatry reported that the drug liraglutide, a treatment for type 2 diabetes, improved certain health measures in people with schizophrenia who were overweight and prediabetic and being treated with the atypical antipsychotics olanzepine or clozapine.
In the 16-week trial, patients received a daily 2 mg injection of liraglutide under the skin or placebo. Liraglutide decreased body weight, improved glucose tolerance, and improved cardio-metabolic measures. Weight decreased by more than 10 pounds on average compared to placebo.
Liraglutide is derived from a human metabolic hormone. It binds to the same receptors as does the metabolic hormone GLP-1, which stimulates insulin secretion.
FDA Approves New Higher Dose of Valbenazine for Tardive Dyskinesia
The US Food and Drug Administration has approved an 80 mg capsule dose of valbenazine (Ingrezza) for tardive dyskinesia (jerky, involuntary movements of the face, especially the mouth and tongue, fingers and body that can be a side effect of antipsychotic medication). Valbenazine, a selective vesicular monoamine transporter 2 inhibitor, was the first drug FDA-approved for tardive dyskinesia. The FDA initially approved a dosage of 40 mg/day in April 2017. The 80 mg/day dose was approved in October 2017.
The new approval was based on a 6-week clinical trial in which 80 mg of valbenazine improved tardive dyskinesia significantly compared to placebo. Improvement continued over 48 weeks of treatment.
Augmentation Strategies for Negative Symptoms of Schizophrenia

In a 2017 article in the journal JAMA Psychiatry, Christoph U. Correll and colleagues reviewed 42 secondary strategies to treat schizophrenia when the primary antipsychotic treatment has an incomplete effect. Many people with schizophrenia show only a limited response to antipsychotic drugs, so additional treatments are often necessary, but currently there are no US Food and Drug Administration guidelines for combination treatment.
Correll and colleagues compiled data from 29 meta-analyses covering 381 individual trials. They found that while the meta-analyses were well done, the quality of the data in the original studies was lacking.
Focusing on Negative Symptoms
However, since the negative symptoms of the illness such as apathy, withdrawal, and blunted emotional response are the hardest to treat, any amount of improvement in this area could be particularly helpful. Read more
Probiotics May Improve Depression As Well As IBS
 A pilot study of people with irritable bowel syndrome (IBS) suggests that taking a probiotic nutritional supplement can improve depression as well as gastrointestinal upset.
A pilot study of people with irritable bowel syndrome (IBS) suggests that taking a probiotic nutritional supplement can improve depression as well as gastrointestinal upset.
In the 2017 study published in the journal Gastroenterology, researcher Maria Pinto Sanchez and colleagues at the Farncombe Family Digestive Health Research Institute found that when those with IBS took a probiotic, their co-occurring depression improved more than it did in people with IBS who took a placebo.
Senior author Premysl Bercik suggested the study confirms that the microbiota environment in the gut affects what goes on in the brain, opening new avenues for the treatment of psychiatric diseases.
The study included 44 adults with IBS who also had mild to moderate anxiety and depression. For 10 weeks, half received a daily dose of the probiotic Bifidobacterium longum NCC3001, while the others received placebo.
After 6 weeks, 64% of the probiotic group saw improvement in their depression, compared to 32% of the placebo group. Functional magnetic resonance imaging (fMRI) showed brain changes associated with the improvement in mood.
The researchers are planning larger trials of probiotics.
