
AiTBS Superior to ECT in Small Study
Researchers Erica Jensen and Nolan Williams reported in abstracts of a paper that they were to present at the 2020 meeting of the Society of Biological Psychiatry in May that daily sessions of accelerated intermittent theta burst transcranial stimulation (aiTBS) over five or more days produced better results in 15 patients hospitalized for depression and suicidality than in matched patients who received electro-convulsive therapy.
AiTBS is a form of repeated transcranial magnetic stimulation (rTMS), in which a magnetic coil is applied to a patient’s scalp, producing electrical changes in the brain.
The aiTBS treatment was delivered to the left dorsolateral prefrontal cortex. It consisted of 1800 pulses per session, at 80% of a patient’s resting motor threshold with a 50-minute inter-session interval.
The patients in the study were matched (for age, gender, and treatment resistance) to patients who were hospitalized and given ECT. Among patients who received aiTBS and were discharged after an average of 8.4 days, there was an 86% response rate and a 73% remission rate. Among the patients who received ECT, who were discharged after an average of 22.3 days, there was a 53% response rate and a 40% remission rate. With further ECT, response and remission rates increased to 73% and 67%. Time to remission was 3.5 days with aiTBS and 31.3 days for ECT. The investigators concluded conservatively, “Our results suggest that aiTBS could have comparable efficacy to ECT, with potentially faster resolution of acute severe depression.”
Editor’s Note: ECT has been the gold standard treatment for severe depression and suicidality and now we may have a platinum comparator. If these findings are replicated, they could represent a paradigm shift in the treatment of severe depression. Hopefully, this novel form of rTMS will be fast-tracked for approval by the Food and Drug Administration (FDA).
Ultrabrief Right Unilateral ECT Similar in Efficacy to Brief ECT with Fewer Side Effects
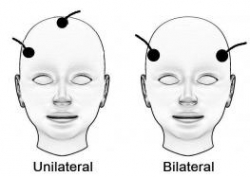 A new meta-analysis suggests that right unilateral ultrabrief electroconvulsive therapy (ECT) may be a better choice than standard brief pulse ECT for the treatment of severe depression. Researchers at the University of New South Wales in Australia led by Colleen Loo say that while standard ECT (with a pulsewidth of 1.0 ms) is recommended when urgency is paramount, ultrabrief ECT (with a pulsewidth of 0.3 ms) is better for patients at risk for cognitive side effects or those who do not require an urgent response. The researchers’ findings were reported in the Journal of Clinical Psychiatry in July.
A new meta-analysis suggests that right unilateral ultrabrief electroconvulsive therapy (ECT) may be a better choice than standard brief pulse ECT for the treatment of severe depression. Researchers at the University of New South Wales in Australia led by Colleen Loo say that while standard ECT (with a pulsewidth of 1.0 ms) is recommended when urgency is paramount, ultrabrief ECT (with a pulsewidth of 0.3 ms) is better for patients at risk for cognitive side effects or those who do not require an urgent response. The researchers’ findings were reported in the Journal of Clinical Psychiatry in July.
Loo and colleagues analyzed the findings of six different studies that compared right unilateral standard brief pulse ECT with ultrabrief pulse ECT and included a total of 689 patients. Standard ECT was more effective, producing more improvement in mood and more remissions, and working faster than ultrabrief ECT. However, standard ECT also produced greater cognitive side effects in every area tested, including thinking, learning and recall, and memory.
(When bilateral ECT is used, the cognitive effects are even worse, and researcher Harold Sacheim and colleagues have reported that the severity of the impairment in autobiographic memory is directly proportional to the number of bilateral ECT treatments a patient received, even when measured one year after the last session of bilateral ECT. This editor (Robert Post) believes bilateral ECT should be avoided if at all possible, as cognitive side effects can occasionally be severe.)
When Loo and colleagues removed nonrandomized trials from the analysis, the differences in efficacy between ultrabrief and standard right unilateral ECT were not statistically significant. Loo told Medscape Medical News that while the differences in efficacy between brief and ultrabrief ECT are minimal, the differences in side effects are greater. Right unilateral ultrabrief ECT works about as well as standard right unilateral brief pulse ECT, but preserves patients’ cognitive function better.
RTMS in the Elderly and After ECT

At the 2015 meeting of the Society of Biological Psychiatry in May, researcher Daniel Blumberger reported to this editor (Robert M. Post) that he has found repeated transcranial magnetic stimulation (rTMS) to be effective for depression in late life. Blumberger noted that it may be necessary to use higher intensity stimulation (i.e. at 120% of motor threshold instead of the usual 110% of motor threshold) in the elderly in order to overcome the gap between the skull and the brain, which can grow with age due to brain atrophy.
Blumberger has also successfully used rTMS as a followup treatment to a successful course of electroconvulsive therapy (ECT), administering rTMS twice a week for up to 66 treatments in a given patient in order to maintain remission of their depression.
ECT versus Drug Therapy for Bipolar Depression
 Electroconvulsive therapy is often considered a primary treatment option for patients with severe bipolar disorder that has resisted pharmacological treatment. Researcher Helle K. Schoeyen and colleagues recently published the first randomized controlled trial comparing ECT (in this case right unilateral brief pulse ECT) with algorithm-based pharmacological treatment in 76 patients with treatment-resistant bipolar depression.
Electroconvulsive therapy is often considered a primary treatment option for patients with severe bipolar disorder that has resisted pharmacological treatment. Researcher Helle K. Schoeyen and colleagues recently published the first randomized controlled trial comparing ECT (in this case right unilateral brief pulse ECT) with algorithm-based pharmacological treatment in 76 patients with treatment-resistant bipolar depression.
The response rate was significantly higher in the ECT group than in the patients who received drug treatment (73.9% versus 35.0%). However, the two treatment groups had similarly low remission rates (34.8% for ECT and 30.0% for pharmacological treatment).
The algorithm-based pharmacological treatment used in the study was based on a sequence of treatments endorsed by researchers Frederick K. Goodwin and Kay Redfield Jamison in their 2007 book Manic-Depressive Illness. A selected treatment was chosen for each participant based on his or her medical history. If the first treatment was ineffective or intolerable, the patient would be switched to the next treatment option. Antipsychotics, antidepressants, anxiety-reducing drugs, and hypnotics were some of the other treatments included in the algorithms.
Patients in the study had previously showed a lack of response to at least two different antidepressants and/or mood stabilizers with documented efficacy in bipolar disorder (lithium, lamotrigine, quetiapine, or olanzapine) in adequate doses for a period of 6 weeks (or until they quit because of side effects).
Editor’s Note: Even when ECT is effective, there is the issue of how to maintain that good response. We previously reported that in a 2013 study by Axel Nordenskjöld et al. in the Journal of ECT, intensive followup treatment with right unilateral brief pulse ECT combined with pharmacotherapy was more effective than pharmacology alone at preventing relapses. Patients who improved after an acute series of ECT (three times/week) then received weekly ECT for six weeks and every two weeks thereafter, totaling 29 ECT treatments in one year.
Other studies of more intermittent continuation ECT have not proved more effective than medication. Thus high intensity right unilateral brief pulse ECT is one option for extending the effects of successful ECT.
IV Ketamine Produces Antidepressant Effects More Rapidly Than ECT
 More and more evidence suggests that drugs such as ketamine that work by blocking the brain’s NMDA receptors can produce rapid-acting antidepressant effects in patients with depression.
More and more evidence suggests that drugs such as ketamine that work by blocking the brain’s NMDA receptors can produce rapid-acting antidepressant effects in patients with depression.
In a recent study by Ghasemi et al. published in the journal Psychiatric Research, 18 patients with unipolar depression were divided into two groups, one that received intravenous infusions of ketamine hydrochloride (0.5 mg/kg over 45 minutes) three times (every 48 hours), and another that received electroconvulsive therapy (ECT) on the same schedule.
Ketamine produced antidepressant effects more quickly than ECT, and these effects were significantly better than baseline for the duration of the study, but not significantly different from those achieved through ECT by the end of the study.
Editors Note: These data continue to add to the already strong findings that ketamine produces rapid-onset antidepressant effects. When and where ketamine should be incorporated into routine clinical treatment of depression remains to be further clarified.
Investigating Relapse after ECT
 Electroconvulsive therapy (ECT) is an effective treatment for patients with treatment-resistant depression, but still many patients relapse after the treatment. Medications can prolong the period of remission, but even so, relapse rates have increased in recent decades (probably at least partly because ECT was once a standard initial treatment but is now only used with those patients with the most difficult-to-treat illnesses.) A 2013 meta-analysis by Jelovac et al. in Neuropsychopharmacology reviewed existing research on relapse and which medications might be able to best prolong remission after ECT.
Electroconvulsive therapy (ECT) is an effective treatment for patients with treatment-resistant depression, but still many patients relapse after the treatment. Medications can prolong the period of remission, but even so, relapse rates have increased in recent decades (probably at least partly because ECT was once a standard initial treatment but is now only used with those patients with the most difficult-to-treat illnesses.) A 2013 meta-analysis by Jelovac et al. in Neuropsychopharmacology reviewed existing research on relapse and which medications might be able to best prolong remission after ECT.
The researchers analyzed 32 studies that each included at least 2 years of followup. In studies from the recent era in which patients received continuation treatment with medication following ECT, 51.1% of patients relapsed within a year, and the majority of those (37.7%) relapsed within the first 6 months after ECT. Among patients treated with continuation ECT, a similar proportion (37.2%) also relapsed within 6 months of the initial ECT treatment. In randomized controlled trials, treatment with antidepressants with or without lithium following ECT halved the rate of relapse within 6 months compared to placebo.
Even with continuing intermittent ECT treatment, risk of relapse remains high, especially within the first 6 months. The authors concluded that maintenance of wellbeing following ECT must be improved.
Editor’s Note: One possibility for prolonging remission is the more intensive continuation regimen using right unilateral ultrabrief pulse ECT suggested by Nordenskjöld et al. in the Journal of ECT in 2013. Continuation treatment with a combination of ECT and medication resulted in 6-month relapse rates of 29% (compared to 54% with medication alone) and one-year relapse rates of 32% (compared to 61%).
Effectiveness of Continuation Right Unilateral ECT Plus Pharmacotherapy Compared to Pharmacotherapy Alone
Different types of ECT
A new study is one of the first to find that after successful electroconvulsive therapy (ECT) treatment for depression, continuation of ECT together with pharmacotherapy was superior to continuation with pharmacotherapy alone. ECT produces a seizure while a patient is under anesthesia. The treatment has been successful in acutely treating many patients with severe depression who have not responded to other treatments. The question remains how to maintain the positive acute effects of ECT for a longer duration.
The new research was published in the Journal of ECT in 2013 by Axel Nordenskjöld et al. Patients with unipolar or bipolar depression who improved after an acute series of ECT (usually given 3 times per week) were randomized to receive either continuing ECT plus pharmacotherapy or pharmacotherapy alone. The ECT continuation group received weekly ECT for 6 weeks and every 2 weeks thereafter for a total of 29 ECT treatments in one year. The pharmacotherapy consisted of antidepressants (98%), lithium (56%), and antipsychotics (30%). Venlafaxine (Effexor) was considered the first choice for medication, and lithium augmentation was offered to all patients (not just those with bipolar depression). Of the participants, 64% had recurrent unipolar depression, while less than 20% had bipolar depression.
Among all the patients who were randomized at the beginning of the study (the intent-to-treat cohort), the one-year relapse rate was 61% for patients treated with pharmacotherapy alone and 32% for patients treated with the ECT plus pharmacotherapy (p=0.036). Relapse rates at 6 months were 54% for the pharmacotherapy alone group and 29% for the group receiving ECT plus pharmacotherapy. Some patients required inpatient care during the trial—36% of the patients in the pharmacotherapy alone group and 20% of those in the pharmacotherapy plus ECT group. There was no evidence of a differential effect on cognition across the two groups. (There is concern that bilateral ECT can adversely affect cognition, especially autobiographical memory, but this is not a concern with right unilateral ECT.)
Various parameters for ECT have been studied. This research used unilateral ultrabrief pulse ECT. These parameters are standard in Sweden, where the study took place, and these results are of particular interest as they differ from a US study that used bilateral ECT with treatments given more intermittently. In that study, in which response to ECT with pharmacotherapy did not differ from response to pharmacotherapy alone, ECT continuation was given in the form of 4 weekly treatments, 4 biweekly treatments and then 2 monthly treatments, and this regimen resulted in a relapse rate of 37% within 6 months (Kellner et al. 2006).
Only one other study in geriatric patients who were psychotically depressed showed superiority of continuation ECT.
Editor’s Note: The take-home message from this study may be that for patients with recurrent unipolar depression who respond positively to a course of right unilateral ultrabrief pulse ECT, continuation of regular ECT plus pharmacotherapy is worth considering over pharmacotherapy alone. While direct comparative studies have not been performed, it would appear reasonable to use weekly ECT for 6 weeks and then every 2 weeks thereafter for the continuation ECT treatment rather than a more intermittent series of treatments as in the studies of Kellner et al. Previous studies have shown that the addition of lithium to antidepressants is superior to antidepressants alone in the continuation phase of ECT (Sackeim et al. 2001), so having lithium in the regimen would also appear useful.
ECT Update: Some good news and some not-so-good news
A 2013 study by Prudic et al. in the Journal of Electro-convulsive Therapy reveals some good and some not-so-good news about ECT. The good news about ECT is that it produced moderate acute remission rates. In this randomized study of ECT treatment, improvement rates were better when patients received right unilateral (RUL) ultra-brief pulse at high doses (6 times a patient’s seizure threshold) than with bilateral (BL) pulse at low doses (1.5 times the patient’s seizure threshold). RUL also has fewer cognitive side effects than BL.
Prudic also found that these acute remission rates were best when antidepressant treatment was begun at the same time as ECT rather than after the end of ECT treatment.
Unfortunately, a previous study by Prudic et al. showed that relapse rates after ECT remain high. Two-thirds of patients relapse in the first six months after ECT. Half of patients who receive antidepressant treatment following ECT relapse within the first six months after their last ECT treatment. Twenty to forty percent relapse in the first month after their last ECT treatment.
In the current study, timing and likelihood of relapse was independent of whether antidepressant treatment was started at the outset of ECT or after the end of ECT. Relapse also did not depend on which pharmacological treatments are used (nortriptyine plus lithium versus venlafaxine plus lithium).
Older patients (average age 55) did better—they relapsed less often than patients with an average age of 45. Patients with unipolar and bipolar depression did not differ in relapse rates.
Previous history of illness did affect relapse. The number of prior antidepressant trials a patient had tried for a current depressive episode (a measure of treatment resistance) was related to how fast they relapsed on follow-up pharmacotherapy after receiving ECT (more antidepressant trials was associated with faster relapse).
Other studies have shown that continuation of ECT treatment is not superior to continued treatment with drugs following ECT treatment.
Editor’s Note: ECT works acutely, but too often its effects do not last long, even with intensive continuation treatment with an antidepressant and lithium. Therefore for patients with highly recurrent illness, its usefulness is largely limited to acute emergencies, such as high risk of suicide or medical deterioration.
There are currently no good controlled studies showing how to prevent depressive relapse after remission with ECT using either drug continuation therapy or maintenance ECT. Greater degrees of treatment resistance are associated with lower rates of both acute remission and faster relapse during follow-up pharmacotherapy.
If a patient is going to have ECT, RUL would be recommended over bilateral, because bilateral ECT is associated with decreases in autobiographical memory even after six months, and these deficits are in proportion to the number of bilateral ECT treatments received.
Alternatives to ECT
Other types of brain stimulation treatments could potentially serve as alternatives to ECT. Read more
RTMS Versus ECT
 We’ve been posting about repeated transcranial magnetic stimulation (rTMS), a treatment in which a magnetic field is applied to a patient’s head, where it is able to affect tissue 2-3 centimeters into the brain.
We’ve been posting about repeated transcranial magnetic stimulation (rTMS), a treatment in which a magnetic field is applied to a patient’s head, where it is able to affect tissue 2-3 centimeters into the brain.
In randomized, controlled, head to head comparisons of electroconvulsive therapy (ECT) and repeated transcranial magnetic stimulation (rTMS), ECT often proves superior, particularly for a more severe psychotic or medically compromised patient. Nonetheless, for a more routine patient with non-psychotic depression, multiple studies have shown approximate equivalence of rTMS and ECT, while rTMS may have a superior benefit-to-risk ratio because it brings less risk of cognitive dysfunction. Thus, given almost equivalent efficacy for some subgroups of depressed patients, and a clear advantage for rTMS in terms of lack of cognitive side effects, this editor/clinician would recommend a course of rTMS prior to a series of ECT for the subgroup of non-emergency treatment-resistant depressed patients.
However, for highly treatment-refractory, severe, and particularly psychotic depression, few treatments appear to approach the efficacy and rapid response onset of electroconvulsive therapy (ECT). ECT as given in the modern era involves anesthesia and muscle paralysis while the patient is mechanically ventilated in order to prevent any damage from muscle contractions during the seizure. Read more
Ketamine Effective in ECT-Resistant Depression
 In an abstract presented at the Society of Biological Psychiatry meeting in May, Lobna Ibrahim and Carlos Zarate of the National Institute of Mental Health reported that intravenous infusions of ketamine were effective in a majority of patients with highly treatment-resistant depression, i.e. even those who had been unresponsive to a course of electroconvulsive therapy.
In an abstract presented at the Society of Biological Psychiatry meeting in May, Lobna Ibrahim and Carlos Zarate of the National Institute of Mental Health reported that intravenous infusions of ketamine were effective in a majority of patients with highly treatment-resistant depression, i.e. even those who had been unresponsive to a course of electroconvulsive therapy.
Editor’s note: Few treatments have been explored for this subgroup of highly treatment-resistant patients, although some have been referred for experimental protocols with intracranial deep brain stimulation (DBS) and others have been successfully treated by Mark George and colleagues at the Medical University of South Carolina with very high intensity rTMS over the left prefrontal cortex (at 130% of motor threshold, 10 Hz stimulation). Further study is needed to determine what follow-up procedures can be used to sustain an acute response to ketamine, rTMS, or ECT for the long term. Read more
