
New Drug Cariprazine Approved for Schizophrenia and Bipolar Disorder
 In late 2015, the Food and Drug Administration approved the new atypical antipsychotic drug cariprazine for the treatment of schizophrenia and mania in adults. The approval followed a series of clinical trials that showed that the drug reduced symptoms of each illness compared to placebo.
In late 2015, the Food and Drug Administration approved the new atypical antipsychotic drug cariprazine for the treatment of schizophrenia and mania in adults. The approval followed a series of clinical trials that showed that the drug reduced symptoms of each illness compared to placebo.
The most common side effects of cariprazine reported in the trials included tremor, slurred speech, and involuntary muscle movements.
Marijuana May Speed Cortical Loss in Boys at Risk for Schizophrenia

In boys, a decrease in the thickness of the cortex is a part of normal maturation. However, according to a recent study, this process is sped up in boys at high risk for schizophrenia when they use marijuana before the age of 16.
Early use of marijuana has been linked to subsequent development of schizophrenia. Schizophrenia begins about 5 years earlier in males than in females, and the male brain goes through more structural changes during adolescence.
A 2015 article by Tomáš Paus in the journal JAMA Psychiatry incorporated data from three studies, which took place in parts of Canada and England and eight European cities. The studies all included magnetic resonance imaging (MRI) scans of the participants, a measure of their genetic risk of developing schizophrenia, and questions about their past marijuana use. In boys at high risk for schizophrenia based on their genetic profile, cortical thickness dropped more among the ones who used high amounts of marijuana before the age of 16 compared to those who did not.
Paus hypothesizes that the development of schizophrenia is a “two-hit process.” People who develop schizophrenia may have an early risk factor, such as their genetic profile or a problem that occurs in utero, and a later stressor such as drug use in adolescence.
Antioxidant NAC Improves Symptoms of Schizophrenia and Bipolar Disorder

N-acetylcysteine (NAC), an antioxidant available without a prescription in health food stores, has shown remarkable effectiveness when added to regular treatments for schizophrenia, bipolar disorder, and the substance abuse that often accompanies these illnesses.
A 2008 article by Michael Berk and colleagues in the journal Biological Psychiatry reported that compared to placebo, 2 grams/day of NAC reduced both positive symptoms of schizophrenia (hallucinations, delusions) and negative symptoms (social withdrawal, difficulty planning and problem-solving). A 2013 study by Mehdi Farokhnia found that 2 grams/day of NAC improved negative symptoms in 42 patients with schizophrenia. Two other studies found that NAC improved deficits in auditory sensory processing in people with schizophrenia.
NAC also improves symptoms of bipolar disorder. A 2008 study by Berk and a 2011 study by Pedro Vieira da Silva Magalhães showed that NAC improved bipolar depression, and a small 2013 study by Magalhães showed that it improved mania in 15 patients. After 24 weeks, 60% of those who took NAC were in remission, compared to 15% of those taking placebo.
NAC is also effective at reducing habitual behaviors such as substance abuse, which is common in patients with schizophrenia and bipolar disorder. Studies have shown that NAC can reduce patients’ use of marijuana, cocaine, alcohol, and nicotine. It is relatively safe with minimal side effects, and fights oxidative stress, which is also common in severe mental illness.
NAC comes in 500mg or 600mg capsules. Dosing typically begins with one capsule twice a day for a week, followed by two tablets twice a day thereafter. As with any recommendations in the BNN, these should not be acted on without guidance from a treating physician.
Brain Inflammation in People at High Risk for Schizophrenia
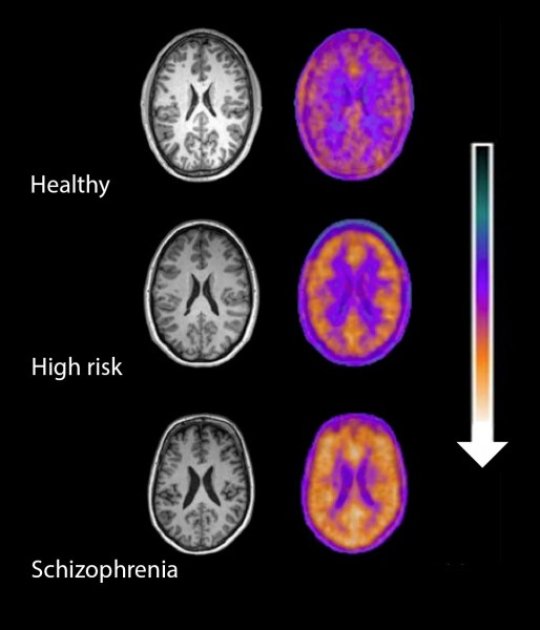
Microglial activity in the brains of people who are healthy, people at high risk for schizophrenia, and people who have been diagnosed with schizophrenia.
A 2016 study by Peter S. Bloomfield and colleagues in the American Journal of Psychiatry used PET scans to compare the activity of microglia, immune cells in the central nervous system, in healthy controls, people with schizophrenia, and those at high risk for the illness. It found that both people with schizophrenia and those at high risk had greater brain inflammation than the healthy controls.
The study was the first to show that microglial activity was elevated in people at high risk (who showed some preliminary symptoms of schizophrenia). The finding had a large effect size.
Microglial activity was also correlated with symptom severity in the high-risk participants. Increased microglial activity was not linked to depression, suggesting that it is specific to the development of psychosis.
These findings resemble those of other recent studies showing increased inflammation in people at high risk for psychosis.
The study suggests that increased microglial activity occurs before a first episode of psychosis. That means it could help identify people who may develop schizophrenia. The findings also suggest that anti-inflammatory treatment could theoretically be used to prevent psychosis.
Schizophrenia: The Importance of Catching It Early

By the time psychosis appears in someone with schizophrenia, biological changes associated with the illness may have already been present for years. A 2015 article by R.S. Kahn and I.E. Sommer in the journal Molecular Psychiatry describes some of these abnormalities and how treatments might better target them.
One such change is in brain volume. At the time of diagnosis, schizophrenia patients have a lower intracranial volume on average than healthy people. Brain growth stops around age 13, suggesting that reduced brain growth in people with schizophrenia occurs before that age.
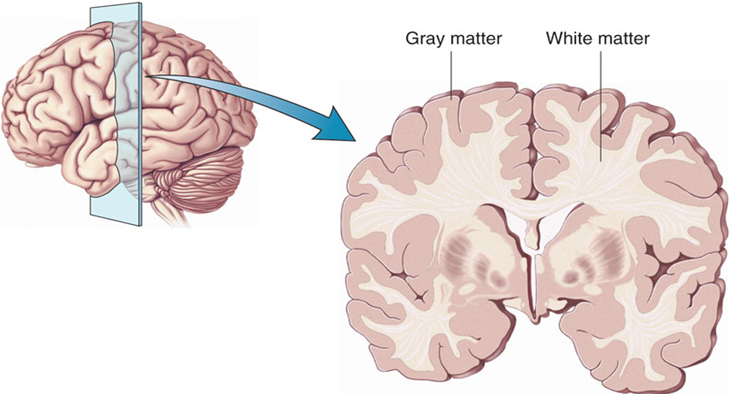
At diagnosis, patients with schizophrenia show decrements in both white and grey matter in the brain. Grey matter volume tends to decrease further in these patients over time, while white matter volume remains stable or can even increase.
Overproduction of dopamine in the striatum is another abnormality seen in the brains of schizophrenia patients at the time of diagnosis.
Possibly years before the dopamine abnormalities are observed, underfunctioning of the NMDA receptor and low-grade brain inflammation occur. These may be linked to cognitive impairment and negative symptoms of schizophrenia such as social withdrawal or apathy, suggesting that there is an at-risk period before psychosis appears when these symptoms can be identified and addressed. Psychosocial treatments such as individual, group, or family psychotherapy and omega-3 fatty acid supplementation have both been shown to decrease the rate of conversion from early symptoms to full-blown psychosis.
Using antipsychotic drugs to treat the dopamine abnormalities is generally successful in patients in their first episode of schizophrenia. Use of atypical antipsychotics is associated with less brain volume loss than use of the older typical antipsychotics. Treatments to correct the NMDA receptor abnormalities and brain inflammation, however, are only modestly effective. (Though there are data to support the effectiveness of the antioxidant n-acetylcysteine (NAC) on negative symptoms compared to placebo.) Kahn and Sommer suggest that applying treatments when cognitive and social function begin to be impaired (rather than waiting until psychosis appears) could make them more effective.
The authors also suggest that more postmortem brain analyses, neuroimaging studies, animal studies, and studies of treatments’ effects on brain abnormalities are all needed to clarify the causes of the early brain changes that occur in schizophrenia and identify ways of treating and preventing them.
Direct Current Stimulation Improves Negative Symptoms of Schizophrenia
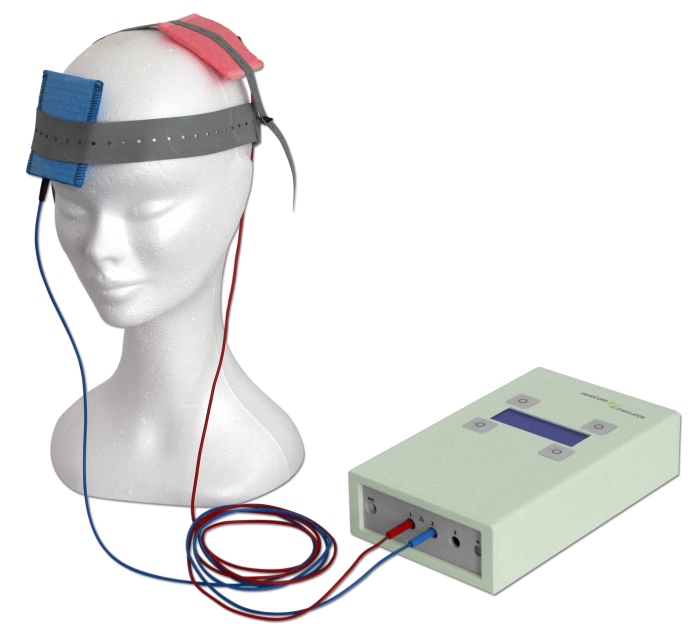 A new double-blind, randomized clinical trial has shown that transcranial direct current stimulation (tDCS) can reduce negative symptoms of schizophrenia. TDCS, a treatment in which an anode and a cathode electrode placed on the skull are used to apply a steady, low-level current of electricity to the brain, has been shown to improve neuroplasticity, such as neuronal remodeling, by depolarizing or hyperpolarizing neurons. People with schizophrenia have neuroplasticity deficits in parts of the cortex, so a few case reports and one previous randomized clinical trial have explored the use of tDCS in schizophrenia.
A new double-blind, randomized clinical trial has shown that transcranial direct current stimulation (tDCS) can reduce negative symptoms of schizophrenia. TDCS, a treatment in which an anode and a cathode electrode placed on the skull are used to apply a steady, low-level current of electricity to the brain, has been shown to improve neuroplasticity, such as neuronal remodeling, by depolarizing or hyperpolarizing neurons. People with schizophrenia have neuroplasticity deficits in parts of the cortex, so a few case reports and one previous randomized clinical trial have explored the use of tDCS in schizophrenia.
The current study, presented by Ulrich Palm at the 2015 meeting of the Society of Biological Psychiatry, included 20 patients with primarily negative symptoms of schizophrenia, such as thought disorders, poverty of speech, and withdrawal. The patients, who had stable medication regimes for at least three weeks, were randomized to receive either a sham procedure or tDCS with the anode over the left dorsolateral prefrontal cortex and the cathode over the right eye. TDCS stimulation was delivered at a current of 2 mA ten times over two weeks. The patients continued to take their medication and also received functional connectivity magnetic resonance imaging (fcMRI) before and after tDCS treatment.
Two weeks following the stimulation, scores on a scale of positive symptoms (hallucinations and delusions) and negative symptoms of schizophrenia had decreased significantly in those who received tDCS compared to the sham procedure. A measure of negative symptoms was significantly lower among the tDCS group throughout the study period and at the 2-week followup. The fcMRI revealed that those who received tDCS had a deactivated cluster in the brain region that includes the nucleus accumbens, the subgenual cortex, and the striatum.
This study suggests that tDCS is a promising treatment for otherwise difficult-to-treat symptoms of schizophrenia.
Maternal Infection During Pregnancy May Increase Risk of Schizophrenia in Offspring
 There is mounting evidence from animal studies and epidemiological research that an infection during pregnancy may increase the risk of schizophrenia in the offspring. A recent study by Alan Brown and colleagues presented at the 2015 meeting of the Society of Biological Psychiatry used a large dataset from the Finnish Prenatal Study of Schizophrenia to compare medical data from the mothers of 777 people with schizophrenia (630 with schizophrenia and 147 with schizoaffective disorder) to data from the mothers of 777 healthy people.
There is mounting evidence from animal studies and epidemiological research that an infection during pregnancy may increase the risk of schizophrenia in the offspring. A recent study by Alan Brown and colleagues presented at the 2015 meeting of the Society of Biological Psychiatry used a large dataset from the Finnish Prenatal Study of Schizophrenia to compare medical data from the mothers of 777 people with schizophrenia (630 with schizophrenia and 147 with schizoaffective disorder) to data from the mothers of 777 healthy people.
The study’s biobank contained blood samples taken from the mothers in early to mid-pregnancy, which the researchers used to determine the mothers’ levels of C-reactive protein (CRP), an indicator of inflammation. Higher levels of CRP were associated with increased risk of schizophrenia in the offspring. When the researchers analyzed the findings by sex of the offspring, the link between prenatal infection and schizophrenia risk was significant in males, but not females. The effect was also stronger among offspring born after their due date than those born at or before their due date.
Atypical Antipsychotics May Slow Loss of Gray Matter in Schizophrenia
Progressive losses in gray matter have been observed in the cortex of people with schizophrenia, and those at high risk for the illness. In the past, studies have shown that the amount of antipsychotics a patient is exposed to is correlated with the extent of their deficits in gray matter, suggesting that antipsychotic treatment could exacerbate gray matter loss.
A new meta-analysis by Antotonio Vita and colleagues in the journal Biological Psychiatry shows that first-generation antipsychotics were associated with greater losses in gray matter compared with atypical antipsychotics, which seemed to slow the loss of gray matter.
The meta-analysis analyzed data from 18 longitudinal studies comparing a total of 1155 patients with schizophrenia to 911 healthy control participants. Magnetic resonance imaging (MRI) scans showed that over time, patients with schizophrenia lost more cortical gray matter volume. The patients’ cumulative intake of any kind of antipsychotic between MRI scans was associated with gray matter losses. But when Vita and colleagues drilled down to find differences between patients taking first-generation antipsychotics and those taking second-generation atypical antipsychotics, they found that patients with higher average daily intake of first-generation antipsychotics had greater losses in gray matter, while patients with higher average daily intake of atypical antipsychotics had less progressive losses in gray matter.
This study is the first to compare the effects of first-generation antipsychotics, which were developed in the 1960s, with those of atypical antipsychotics, which came into frequent use in the late 1980s, on cortical gray matter loss in schizophrenia. While first-generation antipsychotics are associated with the side effect of tardive dyskinesia, involuntary movements of the face and jaw, atypical antipsychotics are most commonly associated with weight gain.
Three studies have randomly assigned patients with schizophrenia to receive either first-generation or atypical antipsychotics. In these studies as well, second-generation antipsychotics were associated with smaller losses in gray matter.
The authors speculate that either second-generation antipsychotics may have neuroprotective effects, or first-generation antipsychotics may have neurotoxic effects. They also suggest that first-generation antipsychotics may not have the capacity to interfere with the natural progression of schizophrenia in terms of gray matter losses.
Future studies may investigate differences between specific antipsychotic medications’ effects on gray matter volume. Vita and colleagues reported that in the analysis, the atypical antipsychotic clozapine was associated with the least loss of gray matter of any medication in the included studies.
Editor’s Note: This study is important because it adds to findings questioning the conclusions of a large National Institute of Mental Health–sponsored study known as CATIE and a meta-analysis by John Geddes published in the journal BMJ in 2000, in which he wrote that “There is no clear evidence that atypical antipsychotics are more effective or better tolerated than conventional (first generation) antipsychotics.” Read more
Solutions for Clozapine-Induced Drooling

Clozapine is a treatment for schizophrenia and treatment-resistant bipolar disorder. Drooling is a side effect for about one-third of people taking clozapine. Here are some treatments that may help reduce it:
1) Botox injected into each salivary (parotid) gland in doses of 50 IU.
2) Ipratropium, either sprayed under the tongue or intranasally. A 2004 case series by Oliver Freudenreich in the Journal of Clinical Psychiatry described sublingual administration.
3) Glycopyrrolate. In a 2011 article in the Annals of Pharmacotherapy, AM Bird described some treatments for clozapine-induced drooling, including glycopyrrolate.
4) The blood pressure drugs clonidine (50–100 mg) or terazosin.
4) Transdermal scopolamine patch. This is typically placed behind the ear to reduce motion sickness, but it also reduces saliva production.
Transcranial Direct Current Stimulation May Improve Cognition in Schizophrenia
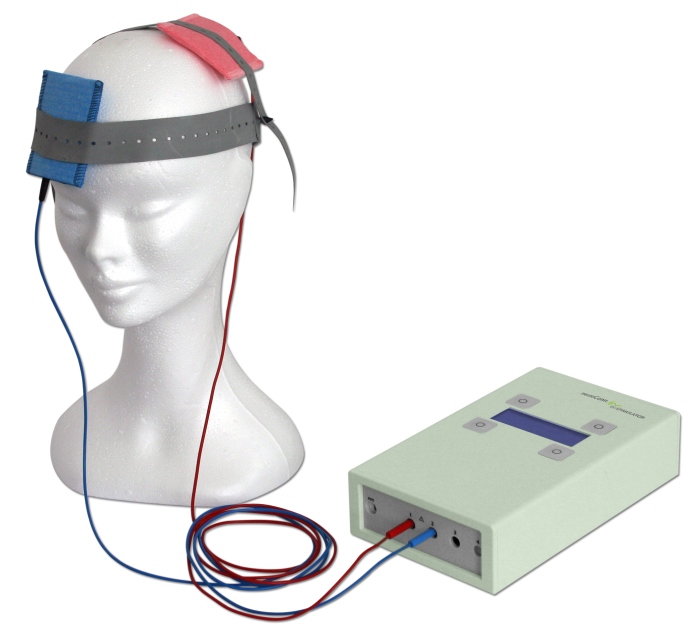 A recent study by Robert Smith and colleagues studied the use of transcranial direct current stimulation (tDCS) in patients with schizophrenia. TDCS is very low level current that has a positive (anode) or negative (cathode) electrode. Anodal stimulation of the cortex is usually associated with positive effects on mood and cognition. Patients received either five sessions of active tDCS for 20 minutes (at 2 milli Amps) or a sham stimulation for the same period. Then, one day after the final session, the patients were measured on a variety of scales for cognition and illness. Patients who received the active tDCS showed more improvements in working memory and attention than patients who received the sham treatment.
A recent study by Robert Smith and colleagues studied the use of transcranial direct current stimulation (tDCS) in patients with schizophrenia. TDCS is very low level current that has a positive (anode) or negative (cathode) electrode. Anodal stimulation of the cortex is usually associated with positive effects on mood and cognition. Patients received either five sessions of active tDCS for 20 minutes (at 2 milli Amps) or a sham stimulation for the same period. Then, one day after the final session, the patients were measured on a variety of scales for cognition and illness. Patients who received the active tDCS showed more improvements in working memory and attention than patients who received the sham treatment.
There was no difference in the two groups’ schizophrenic symptoms, including hallucinations. Smith and colleagues suggest that the improvements in cognition may result from changes to brain connectivity networks, since abnormalities in these networks have been identified in patients with schizophrenia and bipolar disorder.
Replications of this type of study are needed to clarify the effect of tDCS on cognition in schizophrenia, but given the safety and convenience of the procedure, the findings are promising.
