
Suggestions for Physicians Treating Parents with Bipolar Disorder

- Support Pregnant Women with Bipolar Disorder
A. Depression during pregnancy is more common among women with bipolar disorder than among controls–consider cognitive behavioral therapy, omega-3 fatty acids, folate, & rTMS
B. 52% incidence of post-partum depression (3x higher than controls)–Monitor closely and treat accordingly - Ask Your Affectively Ill Patients About Their Children
- Encourage Good Diet and Exercise in These Children
- Encourage Watchful Waiting in Families with Children at High Risk
- If a Child becomes Symptomatic, Suggest:
A. Family Focused Therapy (FFT), or other Family-Based Treatment
B. Low-Risk Interventions Like Nutrition and Sleep Hygiene - If a Child Develops BP-NOS, Encourage:
A. Mainstream Pharmacotherapy
B. Increased Social Support (Family, Friends, Advocacy) - If a Child Develops BP-I, Encourage Ongoing Monitoring & Medication
- If an Adolescent Becomes Manic, Educate About Substance Abuse and Attempt Primary Prevention of a Substance Abuse Disorder
Possible Interventions for At-Risk Children in Addition to Family Focused Therapy

Our editor Robert M. Post recommends that in the absence of good care in the community for children at high risk for bipolar disorder because a parent has the disorder, adult psychiatrists of parents with bipolar disorder who have children with the disorder should fill this gap by treating the children themselves. If the child has only early symptoms, family focused therapy as developed by David Miklowitz would be recommended.
Here are some other suggestions in addition to family focused therapy:
- Good Diet, Exercise, Sleep Hygiene
- Omega-3 Fatty Acids
- Check Vitamin D3 levels and Add Supplement if Needed
- Melatonin for Insomnia
- N-acetylcysteine (NAC) for Irritability (as in studies of children with autism spectrum disorders)
- Folate for Depression and/or Elevated Homocysteine
- Check for Evidence of Inflammation (Increased IL-6 or CRP)
Options with Some Side Effects:
- Minocycline (an anti-inflammatory neuroprotective antibiotic)
Important Reminders from the APA Symposium on Special Topics in Bipolar Disorder

Our editor Robert M. Post served as discussant at a symposium on special topics in bipolar disorder at the 2013 meeting of the American Psychiatic Association. Here are some of the findings that were presented at the symposium.
Michael Gitlin of the University of California, Los Angeles (UCLA) emphasized the importance of treating patients until remission in order to achieve functional recovery and prevent cognitive impairment.
Michael Bauer of Dresden, Germany reviewed data showing that early onset of the illness and long delays to first treatment are important predictors of poor response to treatment.
Mark Frye of the Mayo Clinic discussed the promise of pharmacogenomics to aid in the selection of the best medicine for a given individual (i.e. personalized medicine). Currently the presence of one of a few relatively rare gene variations—HLA-B 1502 (in Asian populations) and HLA-A 3101 (in European populations)—can predict that an individual may develop a severe rash when taking the anticonvulsant carbamazepine. Researcher J. Rybakowski has found that a somewhat common variant in the gene responsible for producing brain-derived neurotrophic factor (the val-66-met allele for proBDNF) is associated with a good response to lithium. This may be explained by the fact that lithium increases BDNF, and this could be crucial in those with the val-66-met allele, which functions less efficiently than the more common and better functioning allele val-66-val.
David Miklowitz, also of UCLA, reviewed data that strongly indicates psychotherapy is effective in the treatment and prevention of bipolar depression. He and Kiki Chang of Stanford University found that family focused therapy (FFT) was effective in treating early syndromes that sometimes lead to bipolar disorder (including depression, anxiety, or BP-NOS) in children at high risk for bipolar disorder because of a family history that includes bipolar disorder in a first degree relative. Yesterday we shared the 8 key ingredients to family focused therapy.
In his discussion, Post emphasized several points from each presentation. Among these was the recommendation by both Gitlin and Bauer that patients use a personal calendar to monitor symptoms and side effects. (We offer an easy download of a personal calendar.)
Post also endorsed Bauer’s emphasis on the need for early intervention, since delay to first treatment is an independent risk factor for a poor outcome in adulthood. (This finding has been replicated in three studies — Franchini et al. in 1999, Post et al. in 2010, and Drancourt et al. in 2012.
Each of these factors and family focused therapy need greater attention in the US, since Post noted that all aspects of bipolar disorder are more difficult for patients in the US compared to those in Germany, the Netherlands, and many other European countries. About two-thirds of the adults with bipolar disorder in the US had onset of the illness before age 19, while in most European countries, only about one-third of adult patients had an early onset. These data are also consistent with the low incidence of bipolar disorder in children at high risk for the disorder because of a parent with bipolar disorder in studies from the Netherlands, Switzerland, and Germany. In contrast, similar studies of children with at least on parent diagnosed with bipolar disorder in the US (by Chang et al., Nurnberger et al., Wozniak et al., and Birmaher et al.) show a higher incidence of the illness. Canadian studies by Duffy et al. and studies of an isolated Amish community in Pennsylvania by Egeland et al. show a low incidence much like the Europeans.
Given the great need for care of children with signs of bipolar disorder in the US and the shortage of child psychiatrists and pediatricians knowledgeable about bipolar disorder, Post recommended that in the absence of other alternatives, adult psychiatrists of parents with bipolar disorder who have children with the disorder should fill this gap by treating the children themselves. If the child has only early symptoms, family focused therapy as described by Miklowitz above would be recommended.
Tomorrow and Friday we’ll share tables with recommendations for the treatment of parents with bipolar disorder and their children.
Family Focused Therapy

Family focused therapy (FFT), developed by David Miklowitz, a professor of psychiatry at the University of California, Los Angeles, has been effective in treating early syndromes that sometimes lead to bipolar disorder (including depression, anxiety, or BP-NOS) in children at high risk for bipolar disorder because of a family history that includes bipolar disorder in a first degree relative. There are 8 key ingredients to family focused therapy.
- Consistent monitoring of the illness and developing an early warning system with a plan for responding if early symptoms emerge
- Stress management
- Development of a relapse prevention plan
- Emphasis on sleep hygiene and the importance of regular sleep patterns
- Work on medication adherence
- Development of self-regulatory skills
- Improvement of family relationships
- Avoidance of substances of abuse
More Evidence That Regular Antidepressants Do Not Work in Bipolar Depression

Psychiatrists most commonly prescribe antidepressants for bipolar depression, but mounting evidence shows that the traditional antidepressants that are effective in unipolar depression are not effective in bipolar disorder. At the 2013 meeting of the American Psychiatric Association, researcher Jessica Lynn Warner reported that among 377 patients with Bipolar I Disorder who were discharged from a hospital, those who were prescribed an antidepressant at discharge were just as likely to be remitted for a new depression than those not given an antidepressant.
The average time to readmission also did not differ across the two groups and was 205 +/- 152 days. Those patients prescribed the serotonin and norepinephrine reuptake inhibitor (SNRI) drug venlafaxine (Effexor) were three times more likely to be readmitted than those not prescribed antidepressants.
These naturalistic data (generated from observations of what doctors normally do and information in the hospital’s clinical notes) resemble those from controlled studies. In the most recent meta-analysis of antidepressants in the treatment of bipolar depression (by researchers Sidor and MacQueen), there appeared to be no benefit to adding antidepressants to ongoing treatment with a mood stabilizer over adding placebo. Randomized studies by this editor Post et al. and Vieta et al. have shown that venlafaxine is more likely to bring about switches into mania than other types of antidepressants such as bupropion or selective serotonin reuptake inhibitors (SSRIs).
In addition, a naturalistic study published by this editor Post et al. in the Journal of Clinical Psychiatry in 2012 showed that the number of times antidepressants were prescribed prior to a patient’s entrance into a treatment network (the Bipolar Collaborative Network) at an average age of 40 was related to their failure to achieve a good response or a remission for a duration of at least six months during prospective treatment.
Editor’s Note: Antidepressants are still the most widely used treatments for bipolar depression, and their popularity over more effective treatments (mood stabilizers and some atypical antipsychotics) probably contributes to the fact that patients with bipolar disorder receiving typical treatment in their communities spend three times as much time in depressions than in manic episodes. Using other treatments first before an antidepressant would appear to do more to prevent bipolar depression. These treatments include mood stabilizers (lithium, lamotrigine, carbamazepine, and valproate); the atypical antipsychotics that are FDA-approved for monotherapy in bipolar depression, lurasidone (Latuda) and quetiapine (Seroquel); and the combination of olanzapine and fluoxetine that goes by the trade name Symbiax.
Evidence from several sources suggests that the SNRI venlafaxine may be a risk factor for switches into mania and lead to re-hospitalizations. Other data suggest that in general, in bipolar depression, augmentation treated with antidepressants should be avoided in several cases: in childhood-onset bipolar depression, in mixed states, and in those with a history of rapid cycling (4 or more episodes per year).
FDA Approves Lurasidone for Bipolar Depression

Last year the BNN summarized two presentations from the 2012 meeting of the American Psychiatric Association showing the antidepressant efficacy of the atypical antipsychotic lurasidone (Latuda) in bipolar depression. Lurasidone was more effective than placebo both when prescribed alone (monotherapy) and when prescribed as an add-on to the mood stabilizers lithium or valproate.
In June 2013, the Federal Drug Administration (FDA) approved lurasidone as both a monotherapy and as an adjunctive therapy with lithium or valproate for bipolar depression. Previously the only FDA-approved agents for bipolar depression were the atypical antipsychotic quetiapine (Seroquel) and the combination of the atypical antipsychotic olanzapine and fluoxetine.
Lurasidone’s precise role in therapeutics remains to be explored, but its side effects profile is of particular interest, as it appears to be less sedating than the other atypical antipsychotics noted above. It also appears to have fewer side effects in the realm of weight gain, cholesterol or triglyceride increases, and increases in blood sugar and insulin resistance.
Psychotherapy Prevents Recurrence of Depression

New research shows that psychotherapy lowers the risk of relapse in unipolar major depression more than “treatment as usual” does, and also heads off depression in children at high risk.
At the 2013 meeting of the American Psychiatric Association, researcher Pim Cuijpers reviewed 32 trials of cognitive behavior therapy, intensive behavioral therapy, and problem solving therapy used for the prevention of depression and found that these therapies were associated with a 21% lower risk of relapse compared to treatment as usual.
There were five critical elements that made these therapies useful: they supported coping with depression, and they included exercise, mindfulness, internet-based cognitive behavior therapy, and problem solving.
Among those who presented at the meeting, Greg Clarke of Kaiser Permanente, Oregon discussed an 8-week course on coping with stress given to a group of adolescents (aged 14 to 16) who had four times the normal risk of developing depression because each had a parent with depression. Clarke found a significant reduction in depression among the adolescents who received therapy compared to controls.
Insomnia can be a precursor to a first depression or to recurrent depression. Cognitive behavior therapy was more effective in improving sleep than a comparative sleep hygiene course.
Researcher Judy Garber presented data showing that cognitive behavior therapy was effective in 13- to 17-year-olds who had a parent with depression and had themselves had a prior depression or were currently sub-syndromal. The effect of the therapy was only significant if the parent was not depressed at intake.
Effectiveness of Continuation Right Unilateral ECT Plus Pharmacotherapy Compared to Pharmacotherapy Alone
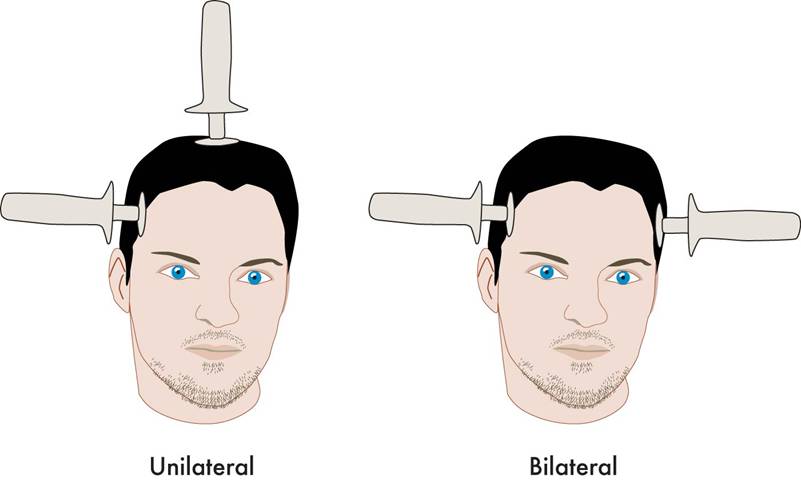
Different types of ECT
A new study is one of the first to find that after successful electroconvulsive therapy (ECT) treatment for depression, continuation of ECT together with pharmacotherapy was superior to continuation with pharmacotherapy alone. ECT produces a seizure while a patient is under anesthesia. The treatment has been successful in acutely treating many patients with severe depression who have not responded to other treatments. The question remains how to maintain the positive acute effects of ECT for a longer duration.
The new research was published in the Journal of ECT in 2013 by Axel Nordenskjöld et al. Patients with unipolar or bipolar depression who improved after an acute series of ECT (usually given 3 times per week) were randomized to receive either continuing ECT plus pharmacotherapy or pharmacotherapy alone. The ECT continuation group received weekly ECT for 6 weeks and every 2 weeks thereafter for a total of 29 ECT treatments in one year. The pharmacotherapy consisted of antidepressants (98%), lithium (56%), and antipsychotics (30%). Venlafaxine (Effexor) was considered the first choice for medication, and lithium augmentation was offered to all patients (not just those with bipolar depression). Of the participants, 64% had recurrent unipolar depression, while less than 20% had bipolar depression.
Among all the patients who were randomized at the beginning of the study (the intent-to-treat cohort), the one-year relapse rate was 61% for patients treated with pharmacotherapy alone and 32% for patients treated with the ECT plus pharmacotherapy (p=0.036). Relapse rates at 6 months were 54% for the pharmacotherapy alone group and 29% for the group receiving ECT plus pharmacotherapy. Some patients required inpatient care during the trial—36% of the patients in the pharmacotherapy alone group and 20% of those in the pharmacotherapy plus ECT group. There was no evidence of a differential effect on cognition across the two groups. (There is concern that bilateral ECT can adversely affect cognition, especially autobiographical memory, but this is not a concern with right unilateral ECT.)
Various parameters for ECT have been studied. This research used unilateral ultrabrief pulse ECT. These parameters are standard in Sweden, where the study took place, and these results are of particular interest as they differ from a US study that used bilateral ECT with treatments given more intermittently. In that study, in which response to ECT with pharmacotherapy did not differ from response to pharmacotherapy alone, ECT continuation was given in the form of 4 weekly treatments, 4 biweekly treatments and then 2 monthly treatments, and this regimen resulted in a relapse rate of 37% within 6 months (Kellner et al. 2006).
Only one other study in geriatric patients who were psychotically depressed showed superiority of continuation ECT.
Editor’s Note: The take-home message from this study may be that for patients with recurrent unipolar depression who respond positively to a course of right unilateral ultrabrief pulse ECT, continuation of regular ECT plus pharmacotherapy is worth considering over pharmacotherapy alone. While direct comparative studies have not been performed, it would appear reasonable to use weekly ECT for 6 weeks and then every 2 weeks thereafter for the continuation ECT treatment rather than a more intermittent series of treatments as in the studies of Kellner et al. Previous studies have shown that the addition of lithium to antidepressants is superior to antidepressants alone in the continuation phase of ECT (Sackeim et al. 2001), so having lithium in the regimen would also appear useful.
A New Target for Deep Brain Stimulation (DBS) for Refractory Depression
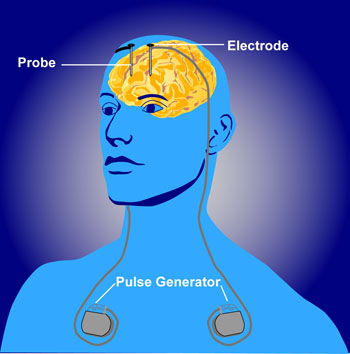 Deep brain stimulation (DBS) is a treatment for illnesses such as Parkinson’s, chronic pain, and depression. In DBS, electrodes inserted in the brain produce electrical impulses. Different anatomical parts of the brain have been targeted successfully using DBS. These include the subgenual anterior cingulate (Area 25), the nucleus accumbens, and the habenula. Now researcher Thomas E. Schlaepfer has found that inserting the n. accumbens electrode deeper and closer to the ventral tegmental area or the VTA (which contains dopamine cell bodies) produces more rapid onset of antidepressant effects (in a matter of days) in a high percentage of patients (7 out of 8 according to one of Schlaepfer’s reports). Stimulation of the nucleus accumbens in the typical location resulted in 50% improvement in 5 out of 10 patients after one year of follow-up.
Deep brain stimulation (DBS) is a treatment for illnesses such as Parkinson’s, chronic pain, and depression. In DBS, electrodes inserted in the brain produce electrical impulses. Different anatomical parts of the brain have been targeted successfully using DBS. These include the subgenual anterior cingulate (Area 25), the nucleus accumbens, and the habenula. Now researcher Thomas E. Schlaepfer has found that inserting the n. accumbens electrode deeper and closer to the ventral tegmental area or the VTA (which contains dopamine cell bodies) produces more rapid onset of antidepressant effects (in a matter of days) in a high percentage of patients (7 out of 8 according to one of Schlaepfer’s reports). Stimulation of the nucleus accumbens in the typical location resulted in 50% improvement in 5 out of 10 patients after one year of follow-up.
Schlaepfer believes that changing the position of the electrode places it in the medial forebrain bundle (MFB), which contains fibers going from the VTA to the nucleus accumbens. Interestingly, when animals are given the opportunity to self-stimulate this area (by pressing a lever that activates an electrode placed in the area), they will, indicating it is rewarding or pleasurable. The same animals will avoid self-stimulating certain other fiber tract sites in the brain.
Schlaepfer’s research was presented at the 2013 meeting of the Society of Biological Psychiatry, and the abstract is available in the Convention Supplement to the journal Biological Psychiatry, Volume 73, Number 9S.
VNS Covered For Reimbursement For Refractory Epilepsy But Not Refractory Depression
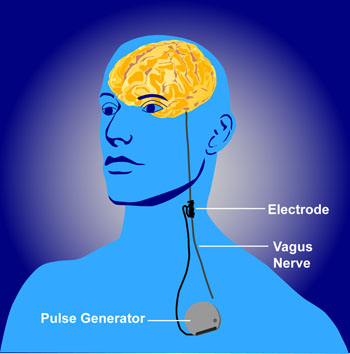 The federal Centers for Medicare and Medicaid Services (CMS) appear to discriminate against people with psychiatric illness. They will not approve the use of VNS (Vagus Nerve Stimulation) for treatment resistant depression among Medicare beneficiaries but have approved it for refractory epilepsy.
The federal Centers for Medicare and Medicaid Services (CMS) appear to discriminate against people with psychiatric illness. They will not approve the use of VNS (Vagus Nerve Stimulation) for treatment resistant depression among Medicare beneficiaries but have approved it for refractory epilepsy.
Vagus nerve stimulation consists of electrical stimulation of the vagus, one of the cranial nerves. The Federal Drug Administration (FDA) has already approved VNS for both illnesses, meaning that it has been judged to be effective and safe in both.
The CMS decision will make it harder for poor patients to access this treatment because it means that Medicare will not reimburse the cost of the treatment.
Cyberonics, the company that manufactures the device used to provide VNS, applied for CMS approval of the use of VNS for depression in 2007 and was rejected, but hoped that the research collected in the intervening years that shows VNS’s efficacy in treatment-resistant depression would be enough to get eventual approval from CMS. They have been rejected again.
Editor’s Note: The data supporting VNS’s efficacy in epilepsy are skimpy and without a large effect size, so it cannot be argued that the quality of data supporting the coverage of VNS for depression is the reason it hasn’t been approved for that purpose. Both epilepsy and depression can be devastating and life altering. To support the use and reimbursement for the same FDA-approved device for one but not the other illness seems worthy of protest.
This appears to be another example of the incongruous use of FDA approval status to deny coverage. Insurance companies and government agencies routinely use lack of FDA approval to deny reimbursement claims for many commonly used drugs and treatments, while at the same time, in cases such as the use of VNS, actual FDA approval is disregarded and considered an insufficient criterion. Having it both ways does not seem to bother the policy makers who appear to put the financial bottom line ahead of ethics, fairness, and good medical care.
